Tomorrow, Australia’s state and federal health ministers will meet for the first time since the May election routed the Morrison government. The national explosion in teenage vaping, driven by access to cheap, highly addictive, sickly-sweet, disposable vapes is on their agenda.
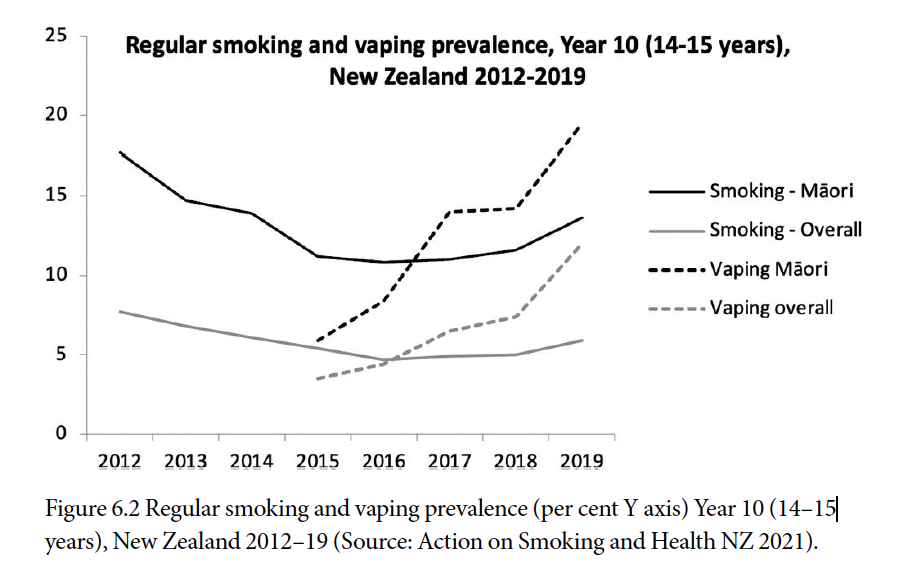
As we saw on Four Corners this week, there can be very few schools across Australia not struggling with the growing epidemic of vaping. Australia hasn’t surveyed teenage vaping in schools since 2017 (a new survey is in the field right now), but in New Zealand the government is now desperately trying to put the teenage vaping genie back in the bottle.
Between 2012 and 2015, prior to the widespread availability of vaping in New Zealand, overall smoking fell by 21% from 6.8% to 5.5% and by 37% from 17.7% to 11.2% in Māori teenagers. But after the advent of vaping, the decline in smoking changed to a growth of 9% between 2015 and 2019, with Māori smoking rising 21%. While this was happening, regular vaping was rising dramatically: between 2015 and 2019, the prevalence of regular vaping rose 173% (5.4% to 12%) and by a roaring 261% in Māori teens (5.4% to 19.5%).
In the USA in 2021, 11.4% of high school students vaped in the last month.
I recently asked my 12-year-old granddaughter what she thought attracted some of her Year 6 classmates to vaping. Instantly she replied “You can get lemonade flavour!” There are more than 15,000 vaping flavours advertised on the web, many of which would not be out of place at a 5 year old’s birthday party.
Australia has 2.7 million people living with asthma. Not one of them uses a flavoured puffer to mask the unpleasant medicinal taste of the salbutamol they typically inhale a few times a day. Why? Because no pharmaceutical regulatory body anywhere in the world allows inhalable flavouring chemicals, with the US Flavouring and Extracts Manufacturing Association warning last year “E-cigarette manufacturers should not represent or suggest that the flavour ingredients used in their products are safe because they are used in food because such statements are false and misleading.”
Daily smokers pull smoke deep into their lungs an average of about 100 times a day. But daily vapers average 500-600, making a mockery of the bizarre denialism spread by some vaping advocates that vaped nicotine is not addictive. As England’s Professor John Britton has said “Inhaling vapour many times a day for decades is unlikely to come without some sort of adverse effect. And time will tell what that will be”

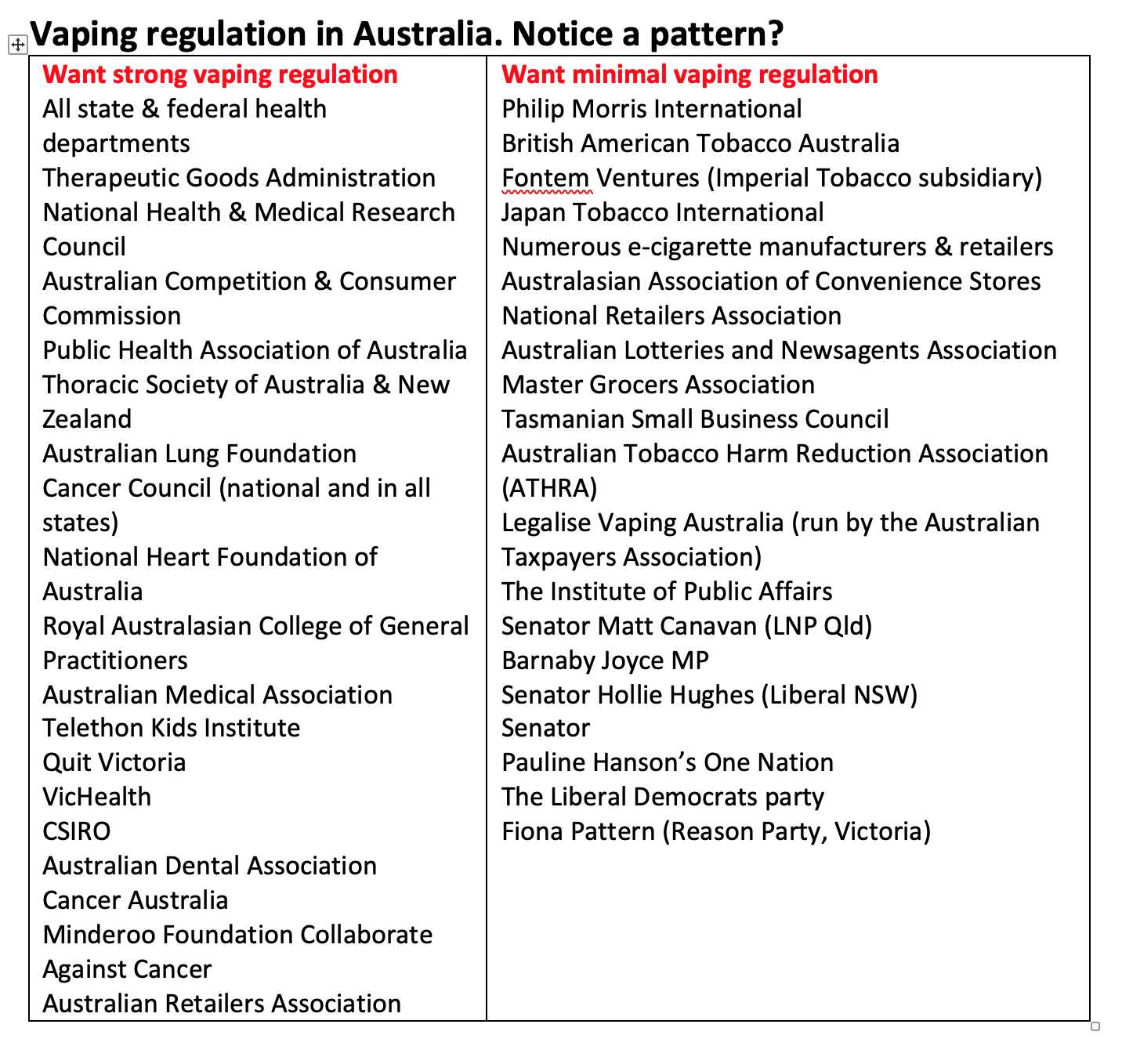
As Four Corners explored on Monday, today’s flood of cheap, disposable vapes can be traced to former health minister Greg Hunt being rolled by a 28-strong backbench revolt led by Queensland National Senator Matt Canavan. Hunt had announced in June 2020 that any adult wanting to vape would need to get a prescription to do so. He also announced it would be illegal (as it has been since July 2019 with cigarettes) to import nicotine-containing vape products. Canavan’s signatories spooked the government and Hunt withdrew the personal import ban.
But the Canavan pro-vaping cabal has been shredded with the departure of Abetz, Falinski, Laming, Wilson and Zimmerman. Its residuals like Hollie Hughes, Canavan and Barnaby Joyce have been rendered political eunuchs by the May election. Hollie Hughes’ performance on Four Corners is causing weapons-grade levels of amusement on Twitter.
Vaping advocates are fond of arguing that because nicotine is freely available in tobacco products, it follows that nicotine for vaping should enjoy at least the same, if not greater accessibility and be freely sold anywhere as a “consumer good” like milk and groceries. This argument has all the integrity of a chocolate teapot. We made every conceivable mistake by failing to regulate tobacco because governments early last century had no idea of today’s 8 million global annual death smoking health toll that took 30-40 years to emerge. Widespread vaping had only been around about 10 years.
Very few kids import their vapes. Why would they bother when they can just walk into the many shops openly selling them, or buy from entrepreneurial kids who buy them in bulk off sites openly advertising them like Facebook Marketplace (search for “fruit” or “vapes”). The vaping chain’s weakest links are retailers and on-line wholesalers. Hitting these is essential to seriously curtailing the tsunami of vapes getting kids. All state governments should introduce seriously deterrent fines for importing and any form of retailing. If corner shops and convenience stores were selling codeine, requiring a prescription, they would be shut down.
Tomorrow, the health ministers should:
- Immediately add disposable vapes to the Prohibited Import Scheme (PIS). This is significantly more urgent from a public health perspective than attempting to close down the Personal Import Scheme for Nicotine Vaping Products (NVPs). This could be achieved very quickly with the stroke of a pen and will cause zero political ructions.
- Harmonise large, significant national increases in fines for commercial quantity importing, wholesaling and retailing of NVPs across all states and territories. These fines and confiscations should be big enough to give serious pause to anyone assuming that their illegal trade can go on, with rare busts costing a fraction of the the profits being earned.
- Cooling agents should be also be immediately added to the exclusion list in the Therapeutic Goods Administration’s TGO 110 (also achievable with a stroke of a pen). These are being used to facilitate vapers inhaling large, highly nicotine doses
- Closing the Personal Import Scheme (PIS) will be a longer game and careful thought should be given to how encouraging the TGA/APHRA/HCCC to focus on telehealth prescription “factories” which are churning out prescriptions often without any acceptable doctor-patient interaction. This could significantly curtail abuse of the PIS by non-legitimate users.
Prescription access via pharmacies selling pharmaceutical grade products can supply adult smokers wanting to switch. Advocates of continuing the open slather access that is now occurring claim Hunt’s prescription access is “prohibition”. By that very silly argument antibiotics, the pill and every other prescribed drug are prohibited too.
Health Minister Mark Butler should seize his first Nicola Roxon moment, and reintroduce the personal import ban. Roxon was lauded internationally for plain packs and Butler can lead the world with workable prescription access not gutted by leaving the front door open to rampant illegal nicotine vape retailing that is addicting a new generation of kids to nicotine who had never smoked.