Recently in The Conversation three commentators proposed a three-pronged template for ending the dominance of illegal tobacco and vapes over legal, taxed and pharmacy-accessed products. Their article was triggered by the release of the latest (2025) AIHW national survey data on smoking and vaping prevalence, where the lowest ever rates were reported for smoking (5.6% daily, 7.8% current).
Let’s look at the evidence and reasoning behind their three proposals: (1) lowering tobacco tax (2) making vapes and other putative reduced risk nicotine products more widely available (3) keeping up enforcement at borders and of stock seizures, fines and closures of illegal retailers.
First, let’s look at their reservations about the integrity of the AIHW data.
They claim that the AIHW has earlier stated that its reports underestimate “actual consumption levels”, meaning that its reports underestimate smoking. But “consumption levels” refer to the number of cigarettes smoked per day, not whether or not people smoke. Reporting lower than true smoking frequency is well known in smoking surveys, where underestimation and rounding down is common.
But there is scant recent evidence of smokers denying they smoke in surveys, particularly when surveys — as with the AIHW’s — are not conducted only face-to-face or via phone where some smokers may feel awkward admitting they smoke.
They also note that the AIHW reported fall occurred at same time that illicit sales “moved underground and were harder to measure”. Surely they realise that the AIHW’s smoking prevalence data report all smoking, regardless of whether this is of legal or illicit products?.
Moreover, authors Jegasothy and Martin have referenced past AIHW data in their government submissions and in their limited academic writing. When useful to their argument, these data are apparently fine, but when inconvenient, they are critical of the data’s integrity.
1 Lowering tobacco tax
I’ve shredded the “reduce the tax” argument many times, like here. But here they go again, advocating an unspecified tax cut and providing no explicit assumptions or modelling. They write “A tax cut won’t close the price gap with the black market entirely. It doesn’t need to. Every dollar the gap narrows weakens the incentive to buy illicit products and the profitability of selling them.”
Illegal cigarettes can be bought for as little as $7 a pack if bought by the carton. If in the highly unlikely and globally unprecedented event that all tobacco excise was removed tomorrow, and manufacturers’ and retailers’ components of price remained at today’s ratios, a pack would cost around $11.50. Most chatter here though has suggested dropping the tax to make a legal pack cost $20-30 instead of the current common $40+. The examples below show on-line carton prices for illicit brands Manchester and Double Happiness of $10.50 per pack.
Illegal prices could also quickly fall far lower than now, with packs in the well-known illicit transit nation of Cambodia for example selling for as little as 34c.
So here they appear to be suggesting that narrowing the price gap will persuade some current illegal tobacco purchasers to ignore any remaining reduced price gap and return to buying more expensive taxed cigarettes.
When pressed, some arguing this way – always without evidence — suggest that many smokers would prefer to be law-abiding and would be willing to pay quite a few dollars more for taxed products if the tax was only reduced.
Here we need only to look at the extent of the cash economy and undeclared sales common with barbers, hairdressers, nail bars, cafes and tradies. The Australian Taxation Office estimates the shadow or cash economy costs Australia approximately $16-$25 billion a year in unpaid tax revenue, with the broader economic impact estimated to be as large as 3% of GDP (exceeding $80 billion in 2025).
Straw-clutching, they also provide a 32 year old (1994) Canadian example of a tax cut with increased enforcement reducing illicit sales. This 2019 World Bank report shows that illegal trade rose again, so that by 2010/11, 32% of Canadian tobacco sales were illicit.
2 Be like Sweden: make vapes and other putative harm reduction products more available
They quote Sweden as an example where policy that embraces harm reduced products has greatly lowered smoking. But Canada and the US are other examples of nations with no legal impediment to the sale of smokeless tobacco and where use of these products is very small and smoking prevalence higher than Australia’s (see “Cherry-picking in Sweden” here). So why only look at Sweden and not mention that it has had low smoking prevalence for many years as well as long-standing comprehensive tobacco control policies?
Illegal vapes are being sold openly in nearly all of the thousands of illegal tobacco outlets in Australia and online with 60% of current 90 day closures in NSW being licensed tobacco retailers. Below is a 70,000 puff vape advertised illegally for $36, less than the cost of one packet of taxed cigarettes. The authors want them to be even more available, as they are in nations like New Zealand, the UK, the USA and Canada. Given how widespread access to vapes is now in Australia, it is difficult to imagine any would-be vaper finding access anything of a problem. And note too that Australian smoking prevalence is also lower than in each of these countries (see table here). So how would even greater access help here?
Early in their article they argue closing down illegal retailers and imports has done little to stem illegal trade. But then they go and recommend it as the third “absolutely essential” of their strategies! This looks like an attempt to walk on both sides of the street. Can please they make up their minds here?
A Sydney closed shop which brazenly reopened was fined $1.18m and permanently closed. There are some 60 more reoffenders in the legal pipeline.
These penalties, which can also include gaol times, are radically changing the risks and costs of engaging in illicit trade in Australia. No country has zero illicit tobacco trade, but Australia is now taking the problem seriously.
The horrendous arson and violence we are witnessing with the extortion and standover tactics being used by criminal syndicates is of course far from unique to their entry into tobacco. Violence is standard modus operandi with organised crime. Extortion and firebombing is also now happening with restaurants, bars and liquor supplies in Victoria, which has nothing to do with excise tax.
Many Australians will tell you that smoking rates here are going up. It’s so obvious, right? Just look at all the illegal tobacco shops that have sprouted across the country selling cigarettes at prices that haven’t been seen here since the late 1990s. Those who smoke the most (low income groups) no longer have the disincentive of high prices to check their smoking. Few kids can afford a $50 pack of legal cigarettes, but many can easily afford $10-$15.
So “everyone knows” that the wheels have therefore fallen off Australia’s historic record of reducing smoking. We are no longer on the front row of the grid of nations who are making smoking history by sending it to record lows. There’s no shortage of ignorant or innocent down-in-the-last shower experts ready to repeat this truth.
Well, hold the press …
The latest national survey of more than 17,500 people aged 14 and over across Australia took part in the National Drug Strategy Household Survey (NDSHS) with data collected from June to December 2025 has been published today by the Australian Institute of Health and Welfare (AIHW).
In 2025, just 5.6% of people aged 14 and over smoked daily, the lowest rate ever recorded since the AIHW began conducting NDSHS surveys in 2001 when the rate was 19.5% (3.5x more than now). In 2022-23 – the last time the national survey was undertaken, the daily smoking rate at 8.3% — an absolute unprecedented fall of 2.7% (and a whopping percentage fall of 32.5%).
Current smoking (at least once per month) is now 7.8% in those aged 14 plus.
Vaping down too
In 2024, the Australian government restricted legal access to vapes to pharmacies, although illegal sales remain widespread. Daily vaping in those aged 14+ (3.6%) has plateaued since from 2022–2023, whereas it was previously increasing.
But current vaping (including less than monthly use) in 18-24 year olds was 14% in 2025, down from an alarming 20.6% in 2022-23, with no increase in smoking as those who opposed pharmacy access often confidently predicted would happen. The same pattern was seen among 14–17-year-olds: current vaping fell from 9.7% in 2022–23 to 6.4% in 2025. Overall, 6% of people aged 14+ vaped at least monthly.
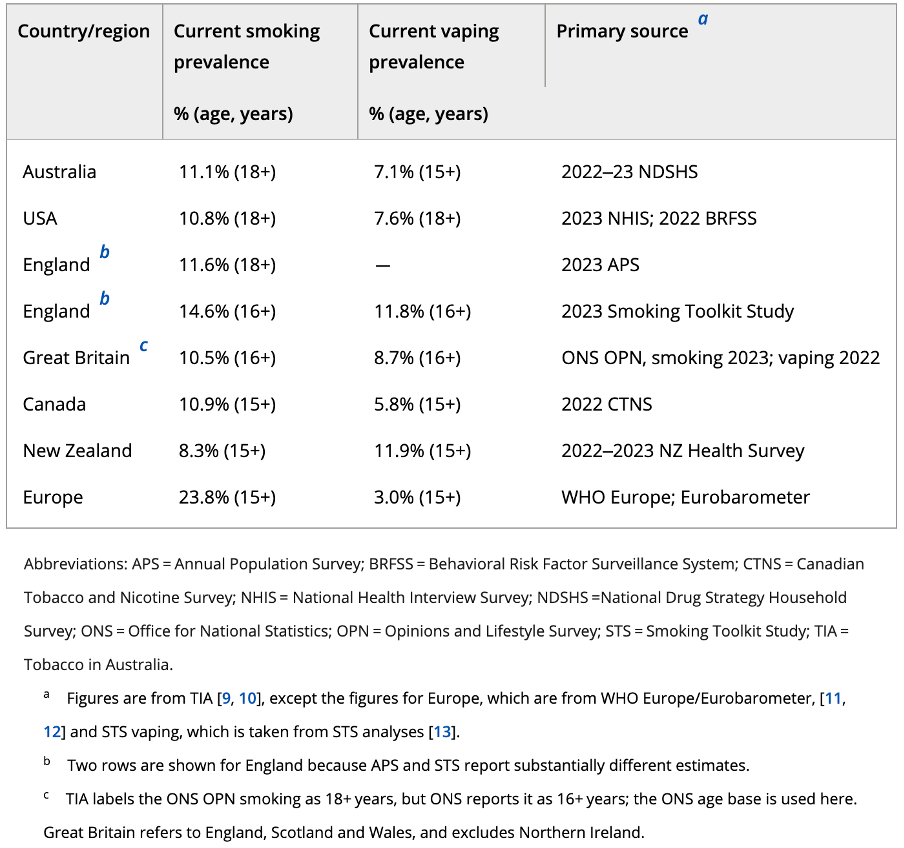
These figures place Australia ahead of other comparable nations with established tobacco control programs on both current smoking and vaping, including the much-vaunted New Zealand rates, which are often held up as the gold standard (see table below). The latest (2024/2025) New Zealand data show 8.3% current smoking (compared with 7.8% in Australia) and 13.8% current vaping, more than double Australia’s rate. (See New Zealand data sources here and here).
Country/region
Current smoking prevalence
Current vaping prevalence
Primary source
% (age, years)
% (age, years)
Australia
7.8% (14+)
6.0% (14+)
2025 NDSHS
USA
9.9% (18+)
7.6% (18+)
2024 NHIS; 2022 BRFSS
England
10.4% (18+)
—
2024 APS
England
14.6% (16+)
11.8% (16+)
2023 Smoking Toolkit Study
Great Britain
9.1% (16+)
10.0% (16+)
2024 ONS OPN
Canada
10.9% (15+)
5.8% (15+)
2022 CTNS
New Zealand
8.3% (15+)
13.8% (15+)
2024/25 NZ Health Survey
Europe
24.1% (15+)
3.0% (15+)
WHO Europe 2024; Eurobarometer 2023
^ Figures are from Tobacco in Australia (TIA) (9,10) except Europe figures, which are from WHO Europe/Eurobarometer, (11,12) and STS vaping, which is from STS analyses.(13) ^^ Two England rows are shown because APS and STS report substantially different estimates. * TIA labels GB ONS OPN smoking as 18+, but ONS reports it as 16+; the ONS age base is used here. Great Britain refers to England, Scotland and Wales, and excludes Northern Ireland. Source for bracketed references shown here
Findings are consistent with other recent surveys
The 2025 NDSHS results are icing on the cake of recent usage surveys conducted in NSW, Queensland, South Australia and with Roy Morgan data from 2022 to 2024. The precise rates of decline vary between studies, but all show that fewer people are smoking.
But … but ….
This news will cause acute dyspepsia in the handful of peripheral commentators who have attracted news spotlights by telling us all that tobacco control is failing in Australia because of high tax and restrictions on the sales of vapes (a bizarre claim because illegal vapes remain highly accessible).
Here are my predictions on how they will try to discredit the new data.
Wastewater analysis shows total nicotine use is up
In June this year the Australian Bureau of Statistics (ABS) published a report on nicotine metabolites in Australian wastewater. The headline finding was that “The quantity of nicotine consumed in Australia increased by almost 40% from 2017 to 2025, with most of the increase occurring since 2021. Population growth over the period 2017-25 was 14%.”
So now that NDSHS data show both smoking and vaping were down in 2025, how can we reconcile this with the ABS nicotine wastewater data?
The ABS report emphasised that “While wastewater data provide reliable estimates of total nicotine consumption, they do not identify which products the nicotine came from.” Importantly, it also states that “It is not possible to discern whether the rise in per capita consumption reflects a rise in the number of people consuming tobacco and/or existing smokers consuming more.”
The NDSHS reports on smoking prevalence, not on nicotine consumption. But the possibility that existing smokers are consuming more nicotine is highly plausible.
Globally, vaping products are undergoing rapid and radical changes. Perhaps chief among these have been the rapid rise in availability and use of nicotine salts. These lower the pH balance of inhaled vapour, producing smoother “throat hit”. Lower pH allows vapers to comfortably inhale much higher nicotine concentrations. AS this has been happening, we have also been seeing the promotion and use of disposable vapes delivering enormous puff counts.
A US analysis found that monthly milligrams of nicotine sold in e-cigarettes increased by 249.2% between February 2020 and June 2024.
Here are examples from a Google search on “50,000 puff vapes”. It’s highly likely that these nicotine geysers are making a substantial contribution to wastewater even among a diminishing number of people who vape.
There’s also evidence of a recent uptick in nicotine replacement therapy, which would add to the volume of nicotine metabolites in wastewater.
Many smokers and vapers questioned for the NDSHS will have lied
These critics will also say scornfully that it’s surely obvious that since a large volume of smokers and vapers are buying illegal products, many will fear trouble if they admit to breaking the law in a questionnaire. This is quite a puerile argument.
The small problem here is that no one has been prosecuted or fined for possessing illegal cigarettes or vapes, unless in commercial quantities. Those buying illegal nicotine products do it openly. The same NDSHS survey asks about illicit drug use where individuals have often been prosecuted and has published data since 2001.
If the AIHW contracted survey team were forwarding information to police gained from their surveys, they would be shut down tomorrow and their directors prosecuted for gross breaches of privacy and misleading conduct.
And had the 2025 findings shown that smoking had risen, it would have been impossible to find any of these critics who would not have fully backed its findings.
Why has smoking kept falling?
Price has always been a major factor explaining both smoking uptake and cessation. Many were therefore concerned that the widespread availability of dirt-cheap cigarettes would put the brakes on the continuing decline in smoking that Australia has enjoyed.
But the task of explaining why smoking has been falling for decades is far more than a simple adding of the sum of the impacts of the all the policies and campaigns we have used to reduce smoking. Trying to disentangle the precise impact of all of them is simplistic reductionist fantasy. In 2017, I wrote this column in The Conversation on the “policy termites” that were slowly eating out the foundations of smoking in Australia and elsewhere. In this review I wrote nearly 20 years ago with Becky Freeman on markers of the denormalisation of smoking, we catalogued a vast range of examples of the ways that the meaning of smoking has changed from something enticing and desirable to something regretted, resented and reviled.
In 2004 some 90% of smokers regretted ever taking it up. This proportion would be much higher today. I’ve never met a smoker who wanted their kids to take it up. The tobacco industry has been repeatedly ranked as ethical bottom feeders in polls on business ethics and trust. It struggles to attract high calibre staff. Most politicians would rather be photographed with the Grim Reaper than enjoying hospitality in a tobacco corporate sporting box.
In the 53 years since Australia introduced its first tobacco control policy (pack warnings), there rarely been a policy advocated to reduce smoking that has failed to be adopted by governments. The tobacco industry and its useful idiot acolytes have lost every policy battle they fought. There is no tobacco manufacturing or legal tobacco farming in Australia, all tobacco advertising and sponsorship has long gone. All indoor workplaces are smokefree. Tobacco packaging is the only consumer product where every square millimetre is regulated. Shops cannot display tobacco.
Today’s wonderful data reflect those successes and the political leadership that made it all happen. Lowering tobacco use and the diseases it causes is the whole point of tobacco control. Australia is well on track to get smoking to down 5% by 2030, and to see the end of smoking by kids. These are simply huge public health achievements.
My colleagues rate Health Minister Mark Butler in the highest pantheon of smart and effective federal health ministers, alongside Nicola Roxon. Australia leads the world in tobacco control. Thank you Mark and your parliamentary colleagues. Stay the course and let’s make smoking history.
Tailpiece 8.50am 17 Jul 2026
Well, we didn’t have to wait long for confirmation of my prediction above that “had the 2025 findings shown that smoking had risen, it would have been impossible to find any of these critics who would not have fully backed its findings.”
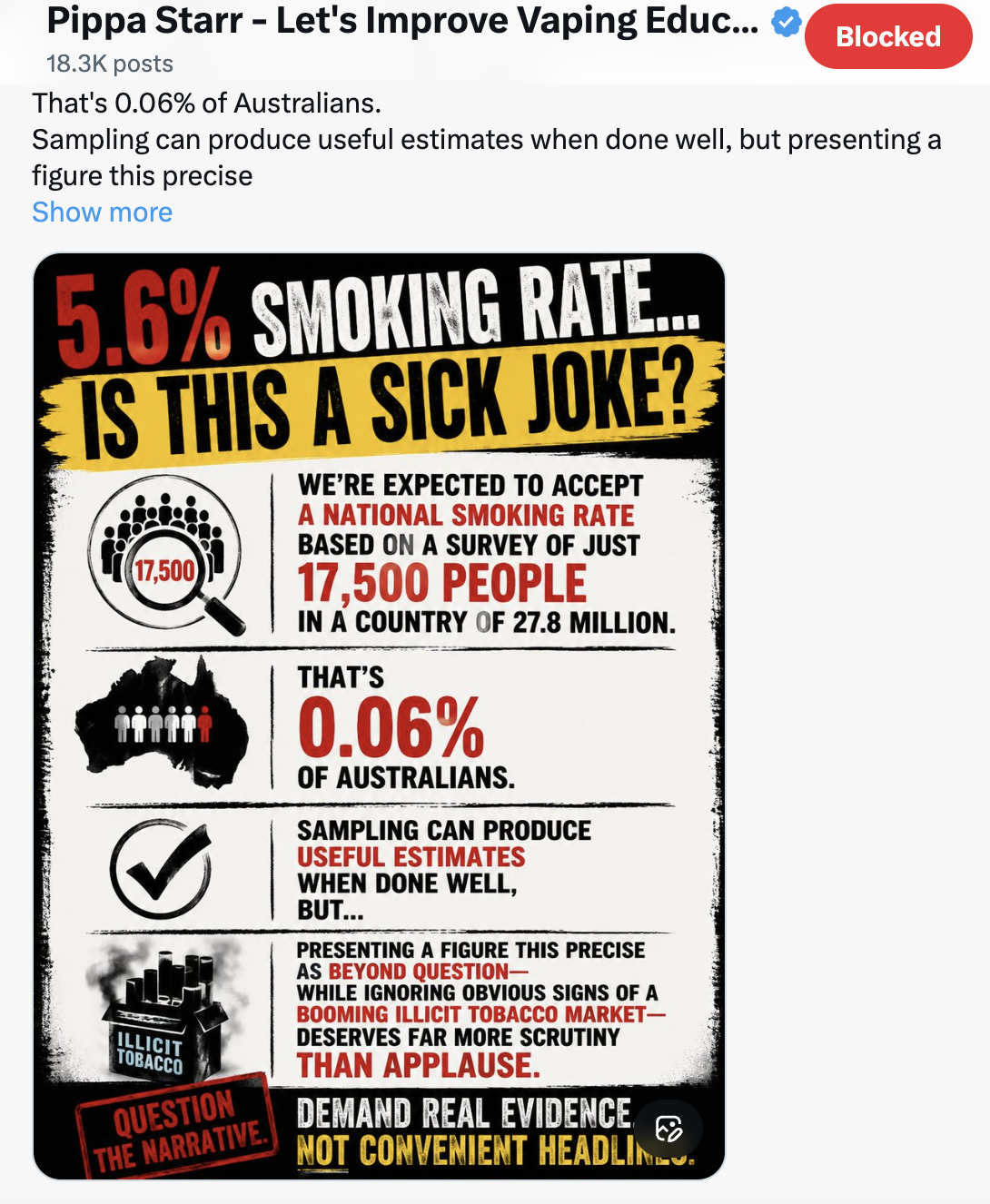
Here’s the inimitable vaping fanatic Pippa Starr on X
And here is a small selection of her past citing of earlier NDSHS data to argue her case. Their data was just fine then apparently, but not now that the findings are inconvenient.
The two giant pillars underpinning vaping advocacy are that (1) vapes are essentially all but as safe as breathing clean air and that (2) vaping is now finally cemented at the highest level of evidence as “the most effective way” we have of quitting smoking. I’ve previously looked at the first of these claims here. This time I’ll look at the effectiveness argument.
Randomised controlled trials: the “gold standard of evidence”
Many smoking cessation advocates megaphone evidence obtained from systematic reviews of randomised controlled trials (RCTs) to argue for the superiority of different drugs or nicotine replacements (especially vapes), over largely unassisted quitting. Quitting cold turkey is routinely cast into a purgatory dungeon as having the lowest level of effectiveness of all ways of quitting. This is despite 70 years of evidence showing that quitting without drugs, aids or professional assistance is and always has been by far the way that most ex-smokers stop on their final quit attempt (see later in this blog). Apparently and preposterously, such quitting is not “evidence based”.
The double-blinded RCT has been elevated to the hallowed zenith of evidence-based medicine. But there are many important ways in which RCTs seriously differ from how therapeutics are used in real world settings, away from the close involvement of RCT researchers. Nowhere is this clearer than with smoking cessation.
When a vaping advocate wants to broadcast the wonderful evidence on vaping, they rarely qualify their claims about RCTs by highlighting or even noting any of these differences. So what does the RCT evidence say and what are these critical differences?
Cochrane evidence on smoking cessation RCTs
The Cochrane library is a global project to pool RCTs on treatments and diagnostics for a wide range of health issues, winnowing those with high quality evidence from those with significant flaws. It has a dedicated sub-section focussed on drugs, nicotine replacement, behavioural and policy interventions to stop tobacco use.
The most recent (10 Nov 2025) Cochrane review of the effect of vaping on smoking cessation measured at (at least) 6 months after the trials concluded that across 104 studies involving 30,366 adults:
“for every 100 people using e-cigarettes to stop smoking 8 to 11 might successfully stop, compared with only 6 in 100 people using NRT, 6 in 100 using e-cigarettes without nicotine or 4 of 100 people having no support or behavioural support [typically advice, counselling etc] only.”
For simplicity here, let’s be generous and take 10 in 100 as the outcome for the e-cigarette group, instead of the stated range 8-11. The Cochrane sentence describes in plain English what is known as the absolute difference in efficacy between vapes, NRT and no support/behavioural support when it comes to quitting. But vaping advocates seldom lead with statements of absolute effect sizes, preferring to use relative effect sizes. Here’s a quick explanation of the important difference between relative and absolute differences, very basic but often misleadingly used concepts at the heart of questions about smoking cessation effectiveness (effectiveness means how something works in the real world; efficacy means how it works in the artificial world of trials).
Absolute vs relative impact
An absolute difference means theexact mathematical difference in event rates (here quit rates) between groups. So if 100 people were to use a smoking cessation medication and 10 quit, while 100 took a placebo and 5 quit, the difference between the two groups at follow-up would be a 5 percentage-point absolute difference. Five more in 100 who used the medication quit (10 altogether) compared with the 5 who used a placebo.
But the relative difference between the two groups is that those on the medication did 100% better than those on placebo (10% being twice as much as 5% — or 100% better). So, if a smoker heard that a particular quit smoking method worked twice as well (ie: 100% better) they would understandably think that here was a no brainer: a way of quitting which was very substantially better that a placebo (or a comparative drug).
So in other words with the latest Cochrane data described above, if you are in a RCT (notwithstanding all the serious caveats set out below) and you used a nicotine vape to try and quit, there would be an absolute positive difference of 4 percentage points higher than if you had used NRT or a nicotine free vape, and 6 percentage points higher than if you had no support to quit or (for example) called a quitline for some counselling.
Flipping this around, this would also mean that a smoker using a nicotine vape would be 90% likely to be still smoking after at least 6 months if they used a nicotine vape; 94% if they used NRT or a nicotine free vape and 96% if they tried to quit pretty much unaided.
So if you were to only express these percentages in relative improvement terms, things will sound so much more encouraging! Now, the improvements from nicotine vaping leap to 66% better than NRT or nicotine free vapes (10/100 v 6/100, the 4/100 difference being 4/6 or 66% better), and 150% better than quitting virtually unaided!
How much more impressive do relative improvements of 66% or 150% sound than the meagre absolute increases of 4 and 6 percentage points?
Veteran vape promoter Alex Wodak had no hesitation in using the heavy ordnance to talk vaping up here when celebrating the release of an earlier Cochrane report:
The Lancet’s policy is that when describing “risk changes or effect sizes … absolute values rather than relative changes” should be used in reports.
Ordinary people typically understand the concept of therapeutic effectiveness as being straightforward. They have many experiences of personally using drugs to alleviate or prevent fever, pain, itching, cramping, nausea, gut problems, contraception, hypertension and more in a very long list.
If they ask a doctor whether a drug being prescribed or recommended “works” they mean works very well: they have high expectations. Few would be keen to use a drug that had a 90% failure rate (as with vapes) when it came to any of these health problems. And they would see trying to quit unaided as well beyond hopeless.
But this is the very low, dismal bar of absolute “success” we find with quit smoking meds, NRT and vaping in RCTs that are widely promoted as the best evidence we can get.
Critical differences between RCTs and real world use
But when RCTs are compared with “real world” studies of how successful vapes are in smoking cessation, the bad news has barely got out of bed.
In RCTs, it is de rigueur to randomly allocate people to the experimental intervention or to a control group and not tell them which group they have been allocated. Those in the experimental intervention group are assigned to receive the active drug or procedure of interest while those in the control group(s) get an inert substance or placebo (a ‘sugar pill’ or saline solution are common). Sometimes there is an extra group being compared: a ‘usual care’ group who have the relevant condition (eg: insomnia, anxiety, migraine). This group are asked to simply continue using the drugs or strategies they normally use for the condition in focus.
With double blinding, the aim is to have neither the trial participants nor the trial research staff know which subjects are in either group. Here, independent third parties are charged with group random allocation and those running the trial are kept in the dark about who is in which group until after the trial has concluded and the data are being examined. Those in the ‘usual care’ group of course know that they are not in the experimental or control group because they are not getting anything.
Enhanced or amplified placebo effects
Allocation is blinded to avoid staff inadvertently letting the cat out of the bag and telling subjects that they are getting the active drug or procedure or the placebo.
This is of critical importance because this knowledge can powerfully influence the expectations of those in a trial. Knowing you are being asked to take a dummy pill (or ointment, patch, lozenge, spray etc) or an established treatment that has been around for decades is understandably likely to deflate expectations of experiencing a positive outcome. This may increase the likelihood of people dropping out of the study (“I know I’m not getting the real thing here, so why bother?”) or adopting other strategies to reduce the problem that inspired them to join the trial to fix the problem. Equally, knowing you really are on the active ingredient intervention may raise your expectations, mirroring those that occur in real world use of a drug.
The asymmetry between knowing you are getting the active drug and knowing you are not may well artificially widen the gap between the performance of the two groups, flattering the performance of the active intervention or drug. This is because of what is termed the enhanced or amplified placebo effect. Belief about whether you are taking an active drug or placebo has been shown to have a substantial impact on therapeutic outcome, with stronger positive expectations resulting in greater therapeutic improvement. This is especially the case when it comes to psychiatric outcomes.
Ideally, those allocated to both intervention and control (placebo) groups should have identical toss-of-a-coin probability of guessing to which group they have been allocated. But many RCTs don’t even test for this “blindness integrity” and when they do, those using the active drug guess correctly far more than by chance,
A 2004 study of 73 nicotine replacement therapy (NRT) trials found only 17 tested for blindness integrity and that in 12 of these 17 subjects (71%) accurately judged treatment assignment at a rate significantly above chance. In a varenicline RCT, those in the varenicline arm were >3 times as likely to believe they were taking varenicline, versus “not sure” and the belief that one had received varenicline was significantly associated with a 5x increase in cessation rate. There’s a similar story with bupropion: Compared to those who guessed “not sure” those guessing they were taking bupropion were more than twice as likely to have been randomized to bupropion.
With nicotine-delivery products (including NRT and nicotine vaping) those with nicotine dependence are thoroughly familiar with the physiological cues they get many times every day when their brain signals to them “feed me, feed me more nicotine please!” So if they have been allocated to placebo group and are still getting those strong sensations, it’s little wonder they often guess they are not getting active nicotine in the trial.
How did the latest Cochrane review handle the issue of blindness integrity?
The Cochrane authors judged all 9 studies in their e-cigarette vs NRT cessation comparison (Analysis 1.1) to be at low risk for “Blinding of participants and personnel (performance bias)”.
Here’s how they get there. The authors say that for randomised studies without blinding, they still rated this domain low risk “if the intervention was compared to an active control of similar intensity”, because they “judged performance bias to be unlikely in this circumstance.” No elaboration of their reasoning was given here.
The lack-of-blinding problem was basically waved through on the assumption that an active NRT comparator neutralises performance bias. But in a field where it is common for trial authors to have spent years publicly and forcefully barracking for e-cigarettes, trial staff enthusiasm and investigator attitudes can shape encouragement, troubleshooting, adherence support, follow-up energy, and participant expectations. So the low-risk performance bias rating for all 9 studies is surely highly questionable.
Combating trial drop out
When RCTs are being planned, calculations should always be made to ensure that sufficient numbers of eligible participants are enrolled to enable enough statistical power to be available to reliably point to any meaningful differences in quit rates. Those running trials must also plan for inevitable dropouts who start a trial but who do not complete it for whatever reasons.
Trial managers are acutely sensitive to the serious threats to scientific integrity, budget blowout and delayed trial completion posed by significant participant drop out. Accordingly both formal ‘tried and tested’ protocols and informal practices are involved in trying to minimise participant attrition. Trial managers use retention strategies which centre around building good relationships with participants to motivate them to remain in trials and maintain their data records. Staff qualities seen as influencing retention include “empathy, being approachable, having a good manner, making trial participants feel appreciated, as well as staff who chat, listen, and answer participant queries, and go ‘the extra mile” … “Having face-to-face contact, or regular follow-up calls with participants, is felt to facilitate building good rapport … Less participant contact possibly hinders retention, as participants do not have a relationship built with trial staff and consequently may not feel as obliged to complete follow-up”
The phenomenon of “research participation effects” (RPE) has largely replaced investigation of issues previously conceptualised as the Hawthorne effect. These constructs are acknowledged as introducing factors which can add important motivations for trial participants to want to please the researchers with whom they have formed positive relationships. Trials often include staff who are PhD candidates who are highly motivated to ensure good trial retention so that their PhD research papers cross that elementary standard of trial integrity and reduce the risk of rejection by journal editors.
Walsh’s 2008 review of 12 smoking cessation trials found subjects were contacted on average 7.1 times across these trials. This level of on-going contact with people who are reminding you and willing you on to keep using a drug for at least the minimum recommended time does not occur when a smoker buys a course of NRT from a supermarket or pharmacy, picks up a script for varenicline, bupropion or cytisine from a doctor or buys a vape.
And here’s the crunch. A review of 7,521 participants in 16 NRT cessation studies found 61% of those in RCTs adhered to their full course of NRT compared with only 26% doing so in population studies. Only 20% of participants in an Australian bupropion trial had completed their full course when followed up. These are radically different levels of adherence, demanding scepticism when RCT results are seamlessly extrapolated to real world relevance.
Smoking cessation treatments are free to trial participants
Again, unlike in real world use, trial participants are provided with free drugs, NRT or vapes. Neither do they pay doctors’ consultation fees where these are relevant. These savings may be particularly attractive to those on low incomes and may positively bias their volunteering in trials. With illegal vapes in Sydney today costing $70-90 for rechargeable products and $50-60 for non-rechargeables depending of the number of puffs obtainable, free vapes will motivate some smokers but represent an unrealistic factor.
RCT subjects are often paid
And again, unlike real world purchasers of quit smoking products, subjects in RCTs are almost always compensated for any expenses incurred in their participation. These includetravel expenses, parking, meals during study visits, accommodation if required and compensation from time away from work. “General inconvenience” payments are also common. Research ethics committees generally will not approve payments that might inordinately influence trial participation “just for the money”. But again, those on low incomes may be attracted to trials and more motivated to see them through even where “general inconvenience” honoraria may be only a few hundred dollars.
Eligibility criteria Ideally, those enrolled in trials should mirror as closely as possible the characteristics of smokers in the population. Some of these are very well established with over-representation in smokers of social disadvantage (low income, education) and higher mental health problem rates than in the general community. This data linkage study of a sample of 1.5m Danish people (1995-2018) found 80% of the population had a history of treatment for a mental health disorder in a hospital setting, from general practitioners or private psychiatrists.
But those running trials prune out participants prior to trial commencement who can be expected to have unacceptable likelihoods of dropping out of the trial, fail to follow the expected procedures and contacts with the researchers or who live in situations where they are hard to contact.
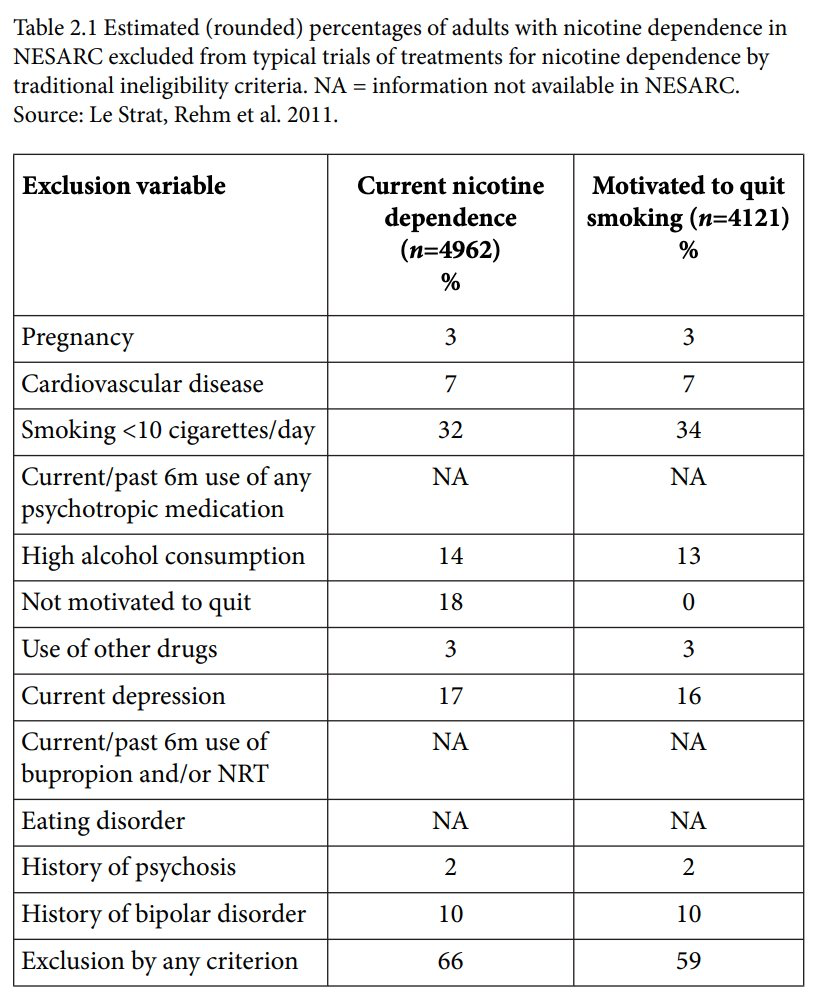
In this review of exclusions from smoking cessation trials, 66% of those with nicotine dependence were excluded and 59% of those motivated to quit were rejected. In the table below the two largest criteria were smoking less than 10 cigarettes a day and insufficient motivation to quit. This is in spite of recommendations for light smokers to use medications and efforts to promote medication use in unmotivated smokers as part of pre-quittng or “preparation to quit” interventions, developments often promoted by pharmaceutical companies.
This US study found 36% of 1206 smokers screened for smoking cessation trial were deemed ineligible for reasons that included serious mental illness, alcohol and drug issues. While 24% of Caucasians were ineligible, 42% of African Americans were excluded.
A review of reviews on 279 RCTs of smoking cessation using pharmacotherapies found 18.3% explicitly excluded participants with any MHDs (mental health disorders), 54.5% conditionally excluded based on certain MHD criteria and 27.2% provided insufficient information to ascertain either inclusion or exclusion. The authors concluded that “smokers with MHDs are not sufficiently represented in RCTs examining the safety and effectiveness of smoking cessation medications.”
In summary, when we add the widespread culling of those less likely to fully participate throughout a smoking cessation trial to the known radically lower levels of treatment adherence as described above, we are looking at serious differences between those participating in trials and those independently using quit smoking aids in real world, totally unsupervised contexts.
Collectively, these differences are likely to significantly flatter the communicated success rates for vaping (and any quit smoking med) promoted from RCTs compared with real world outcomes.
Defenders of RCTs here counter that because trial outcomes are typically calculated using intention-to-treat (ITT) analysis, that RCT outcomes always take attrition into account. ITT analysis involves considering the outcomes of all participants “according to their original assigned treatment group, regardless of whether they actually received the treatment, or dropped out”.
But as discussed above, this does not consider the intense efforts undertaken in RCTs to retain trial participants and to initially screen them to preclude those with known propensity to drop out or with other factors known to be associated with poot outcomes. These collectively introduce important biases into RCTs that make those participating very different and have very different experiences to random cross-sections of smokers trying to quit in the real world.
Longitudinal cohort and population studies
My 2023 (open access) book Quit Smoking Weapons of Mass Distraction(see from pp 185-198) summarises longitudinal population cohort studies on the success of vaping in quitting. It looks also at the question of whether nations with widespread, open-slather vape access have lower smoking prevalence than those where vapes are more restricted or even banned.
Longitudinal cohorts show a similar desultory performance to RCTs, with by far the most common experience of vaping by smokers over several years of follow-up being continuing smoking and vaping (dual use) and abandonment of vaping while smoking continues (see the above pages my book for details).
And when it comes to asking whether nations with now over a decade of widespread liberal access to vapes have plummeting smoking prevalence compared with those with stricter controls, the answer is similarly mostly negative. On this, our recent piece in Addiction shows that with the exception of New Zealand, there is very little difference in smoking prevalence between the five nations shown below nor any obvious relationship between the prevalence of vaping and that of smoking.
“A few quit smoking on their own. Good. But most don’t”
Earlier, I noted the denigration of unassisted quitting as the low water mark of useful ways of quitting. The Australian Department of Health notes that “While quitting cold turkey may not work for everybody, many smokers quit smoking this way.” This is quite an understatement (see here). Wodak’s statement is flagrantly, stonkingly incorrect and suggests he has little understanding of population-wide smoking cessation.
The reputation of unassisted quitting (cold turkey) for having a poor success rate derives from a research obsession with evaluating the outcome of individual quit attempts, rather than taking a population perspective on how large numbers of former smokers stopped smoking on their final, successful attempt.
If we ask “which method of quitting has the best success rate per quitting attempt?” common assisted quitting methods perform better than unassisted attempts. But if we instead ask, “For every 1000 former smokers, what method of quitting has produced the most quitting numbers?” unassisted cessation always wins the prize. What this obsession with success rates rather than with success numbers camouflages is that population attributable quit volumes are a product of success rates multiplied by the number of smokers using various methods. And here, there is daylight between smoking trying to quit without assistance and any (and sometimes all combined) other quit strategy.
Other blogs in this series:
Vaping theology: 1 The Cancer Council Australia takes huge donations from cigarette retailers. WordPress 30 Jul, 2020
Vaping theology: 2 Tobacco control advocates help Big Tobacco. WordPress 12 Aug, 2020
Vaping theology: 3 Australia’s prescribed vaping model “privileges” Big Tobacco WordPress Feb 15, 2020
Vaping theology: 4 Many in tobacco control do not support open access to vapes because they are just protecting their jobs. WordPress 27 Feb 2021
Vaping theology: 5 I take money from China and Bloomberg to conduct bogus studies. WordPress 6 Mar, 2021
Vaping theology: 6 There’s nicotine in potatoes and tomatoes so should we restrict or ban them too? WordPress 9 Mar, 2021
Vaping theology: 7 Vaping prohibitionists have been punished, hurt, suffered and damaged by Big Tobacco WordPress 2 Jun, 2021
Vaping theology: 9 “Won’t somebody please think of the children”. WordPress 6 Sep, 2021
Vaping theology: 10: Almost all young people who vape regularly are already smokers before they tried vaping. WordPress 10 Sep, 2021
Vaping theology: 11 The sky is about to fall in as nicotine vaping starts to require a prescription in Australia. WordPress 28 Sep, 2021
Vaping theology: 12 Nicotine is not very addictive WordPress 3 Jan 2022
Vaping theology 13: Kids who try vaping and then start smoking,would have started smoking regardless. WordPress 20 Jan, 2023
Vaping theology 14: Policies that strictly regulate vaping will drive huge numbers of vapers back to smoking, causing many deaths. WordPress 13 Feb, 2023
Vaping theology 15: The government’s prescription vape access scheme has failed, so let’s regulate and reward illegal sellers for what they’ve been doing. WordPress 27 Mar 2023
Vaping theology 16: “Humans are not rats, so everybody calm down about nicotine being harmful to teenage brains”. WordPress 13 Jul, 2023
Vaping theology 17: “Vaping advocates need to be civil, polite and respectful” … oh wait. WordPress 3 Oct, 2023
Vaping theology 18: Vaping is a fatally disruptive “Kodak moment” for smoking. WordPress Oct 30, 2023
Vaping theology 19: Vaping explosions are rare and those who mention them are hypocrites. WordPress 17 Nov, 2023
Vaping theology 20 : Today’s smokers are hard core nicotine dependent who’ve tried everything and failed – so they need vapes. WordPress 14 Dec, 2023
Vaping theology 21: Australia’s prescription vapes policy failed and saw rises in underage vaping and smoking. WordPress 10 Jan, 2024
Vaping theology 22: “Prohibition has never worked at any point for any other illicit substance”. WordPress 17 Mar 2024
Vaping theology 23: “84% of the Australian public are opposed to the way the government will regulate vapes” WordPress 2 Apr, 2024
Vaping Theology 24: “Tobacco control advocates are responsible for vape retail store fire bombings and murders. WordPress 27 May, 2024
Vaping theology 25: Vaping is as harmless as breathing in stream. So everyone relax. 10 tenets of vaping harm denial.WordPress 10 Mar, 2026
Vaping theology 26: “If Australia allowed vapes to be sold openly, this would lower smoking prevalence and kill illegal tobacco stone dead” WordPress 5 Jun,2026
Of all the arguments flung at public health over the 50 years I’ve worked in it, the claim that “everyone knows prohibition doesn’t work” has few rivals on the podium of insults. It’s fraternal twin barb, the odious, interfering “nanny state” epithet, often walks hand-in-glove with the enemies of prohibition.
I got a confused post recently telling me that the illegal tobacco problem in Australia was caused by prohibition which “never works”. Last time I looked, legal tobacco was on sale in every supermarket (except Aldi), corner store, service station, newsagent, tobacconist and many more. So prohibition clearly was not to blame, but anyway … just put it out there anyway!
“Works?”
Those beloved of this meme rarely explain what they mean by “hasn’t worked”. Do they mean that any ban which is ever ignored by even a tiny minority has therefore failed? Or is the only acceptable bar here, one of a ban eradicating eternally every last instance of a problem?
Slavery began to be outlawed in the nineteenth century. It remains legal in Afghanistan under the Taliban with the International Labor Organisation estimating that 50 million live in illegal slavery today around the world. So put your hand up if this mean that the prohibition on slavery has failed and so should now be abandoned.
“Everyone knows” US alcohol prohibition failed
Most claiming that prohibition doesn’t work point to the example of alcohol prohibition in the USA. Alcohol and drugs expert Professor Wayne Hall from the University of Queensland commenced his 2010 (pay-walled) review in Addiction of the lessons to be learned from alcohol prohibition in the USA with “ ‘Everyone knows’ that national alcohol prohibition in the United States between 1920 and 1933 was a quixotic and failed social experiment”.
In his erudite myth-busting review, Hall examined this factoid (unreliable information that is reported and repeated so often that it becomes accepted as fact) and its implications for policy debates about “bans” on alcohol. He concluded “It is incorrect to claim that the US experience of National Prohibition indicates that prohibition as a means of regulating alcohol is always doomed to failure. Subsequent experience shows that partial prohibitions can produce substantial public health benefits at an acceptable social cost, in the absence of substantial enforcement.”
His review and this piece suggest that prohibition was associated with a number of positive social and economic changes while it lasted, and that the almost universally accepted “fact” that it caused widespread growth in the black market for alcohol and in associated crime and corruption may in fact have been phenomena only documented for a small number of US cities. But most people just know it was an unmitigated failure cross the USA.
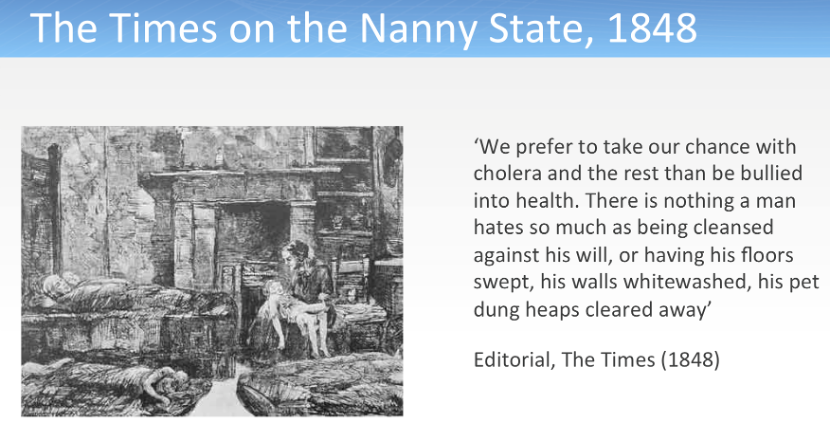
Outrage about prohibitions and the nanny state has a long history
Attacks rained down on Edwin Chadwick, the architect of the first Public Health Act in England in 1848. He proposed the first regulatory measures to control overcrowding, drinking water quality, sewage disposal and building standards. After he was sacked for his trouble an editorial in The Times gloated: ‘We prefer to take our chance with cholera and the rest than be bullied into health. There is nothing a man hates so much as being cleansed against his will, or having his floors swept, his walls whitewashed, his pet dung heaps cleared away’. And yet on the 150th anniversary of the Public Health Act a British Medical Journal poll saw his invention of civic hygiene, and all of its regulations, voted as the most significant advance in public health of all time.
In February 1985, The Age reported that at least three Australian children had been disemboweled in the past two years after sitting on swimming pool skimmer box covers shaped like children’s seats. Before the advent of mandatory shatterproof safety glass for showers, over the years many suffered major lacerations and occasionally died after bathroom accidents. Before 2008, it was legal for fast buck retailers to sell children’s nightwear that could easily catch fire: many children were hideously burnt and scarred for life. Random breath testing was first introduced in 1976, to the chagrin of the Australian Hotels Association. In NSW it was followed by “an immediate 90% decline in road deaths, which soon stabilized at a rate approximately 22% lower than the average for the previous six years”.
These are just four of many examples of changes to laws, regulations, mandatory product standards and public awareness campaigns that were introduced following lobbying from health advocates. With these, as with nearly every campaign to clip the wings of those with the primitive ethics of a cash register, there was protracted resistance. I was a board member of Choice magazine for 20 years, and lost count of the number of times manufacturers staunchly resisted voluntarily making changes to their dangerous, ineffective or substandard products.
Tim Wilson MP
These bans and brakes on personal and commercial freedoms are routinely ridiculed as the interventionist screechings from that reviled harridan, the Nanny State. And the cathedral of the anti-nanny state in Australia has long been the Institute of Public Affairs (IPA). One of its early high priests in Australia was Tim Wilson, now Liberal Member for Goldstein, who pumped out an incontinent flow of the doctrine regularly in opinion pages and interviews.
In May 2013, Wilson, Australia’s champion of contemporary pet dung heap rights, railed that “Nanny state critics understand that incremental attacks on our freedom to choose are single steps down a longer road to remove individual choice and responsibility.” He wrote of the “rising groundswell of Australians who are sick of increasing local, state and federal government regulations of their choices”; denied that people like him want to “selfishly put their wants above the safety and happiness of others”; that we should all “learn to manage risk through our choices” and that it is not “the job of government to coddle us from the world’s evils, avoid risk and use taxes, laws and regulations to either steer or direct our behaviour.”
Those like Wilson opposed to state intervention in markets subscribe to often unarticulated social Darwinist values that imply that those with the misfortune to be killed, injured or made chronically ill by their participation in untrammeled marketplaces had it coming to them. The unregulated marketplace and community is a kind of noble jungle where the fittest survive thanks to their better education and judgment in their consumer choices, their better ability to pay for superior, less dodgy products and to keep up repairs on their cars and homes, and to get employment in work that is not dangerous or toxic. Children living in poorer housing near busy roads in the leaded petrol era, had only their parents to blame for their lead-lowered IQs: they didn’t have to live there! When a toddler drowned in a backyard pool before mandatory pool fencing laws, it was the fault of the feckless parents for not being more vigilant, and nothing to with failure of government to mandate the cost of a fence as part of the cost of a pool. When kids ingested lead or other heavy metals from dodgy toys when these were legal, their parents should have just done their homework and not bought them.
Those who can’t keep up find their way into national health statistics where across almost every area of public health, the poor and less educated have higher rates of disease, injury, major disease risk factors and death.
Below is a big list of nanny state coddlings and protections that a then profoundly ignorant Wilson would have said are “rarely supported by credible research”. I stopped at 150 and could have doubled, tripled or even quadrupled the list. We don’t hear much from the IPA and its ilk on any of these because they are all immensely popular, taken-for granted safeguards on our health, safety and quality of life. Other countries are climbing over themselves to emulate many of these as best practice. Australia is one of the healthiest nations on earth. The precious freedoms that they “erode” are almost always trivial and the industries that were regulated (with some exceptions like asbestos) reluctantly rolled over and still make money from safer products and procedures. No one cares less that their “choice” to buy leaded petrol has been removed. Only the most rapacious libertarians swoon at the unregulated, let-it-rip free market that would wind back the clock of civil society many decades if unleashed by their ideology.
So a public invitation to the IPA, Pauline Hanson and her ilk: which of these 150 heinous intrusions on people’s freedoms and the right to unbridled commerce have not “worked” and which does it wish to see abolished?
The regulations and laws below sometimes are explicit about prohibitions. But all set out what must happen for the standard to be operational. In doing so, each law, standard and regulation this sets up a prohibition on what would not be met if the standard was breached. So for example, compulsory third party motor vehicle injury insurance prohibits not having this insurance if you are a licensed driver.
Finally here is a list of 74 specific and categories of goods which are prohibited from import into Australia. It includes laser pointers, flick knives, body armour, chemical weapons, dangerous breeds of dogs, radioactive substances and mace. There are doubtless advocates for free access to all of these.
James Martin is a Deakin University criminologist with a modest research track record in the tobacco control field. Of his 44 publications listed in Google Scholar, just five concern tobacco or vaping, with only two of these being published in peer reviewed journals. These five have received all of nine citations, with two being self-cites.
This background is relevant to his recent piece in Michael West Media, where he knits a loose thread between the current criminal tsunami of illegal tobacco and vape sales in Australia, Sweden’s falling smoking rates, Australia’s “punishment” of the tobacco industry, our alleged failure to reduce tobacco use, the failure of law enforcement to stem illicit sales and the heinous cruelty to the disadvantaged he says high tobacco prices cause.
His piece there provides just one reference to support his assertions. So let’s walk through how these stand up.
Tobacco control “harms poor smokers”
Martin argues that the Australian government has “abandon[ed] nicotine consumers, disproportionately some of our most vulnerable citizens, to early disease and death – an abominable moral calculation” because of instead of allowing vapes to be sold almost anywhere, it has confined legalised access to vaping through pharmacies to control the open supply of vapes to kids by self-described law-abiding convenience stores, tobacconists and vape shops.
While 2,358 pharmacies have dispensed over-the-counter vapes, and the government fully subsidises prescribed smoking cessation meds to low income health card holders, the unabated supply of cheap illegal, flavoured vapes by criminals continues to undermine the same potential of pharmacy access that we see year in and out when nearly all of us participate in the 440m annual visits to pharmacies to pick up 331m annual prescribed medicines.
If crime syndicates were also brazenly selling these medicines in every suburb to walk-ins without prescriptions, saving low income customers lots of money, should we applaud their public spirited service to the poor and let them get on with it? Or would we instead applaud swift and serious government effort to close this down and uphold the rule of law? I know what I would do.
And Big Tobacco — apparently the new white knights of health promotion – according to Martin now “grasps that its future, at least in the West, lies in selling nicotine without the smoke.” This is the same Big Tobacco which a decade on from entering the vaping and smokeless markets, still derives over 80% of its income from cigarettes with not one company setting a date to get out of tobacco.
Global Tobacco Industry Revenue Breakdown
Cigarettes: 83% to 88% of global sales
Smokeless tobacco: ~11%
Cigars: ~2%
Otherproducts (e.g., vapes, pouches): ~3%
Company-Specific Financials
British American Tobacco (BAT): Reported that combustible products (primarily cigarettes) generated 80% of total global revenue.
New Category Products: “Next-generation” items make up 13.3% of BAT’s revenue.
Traditional Oral & Other: These account for the remaining 6.7%.
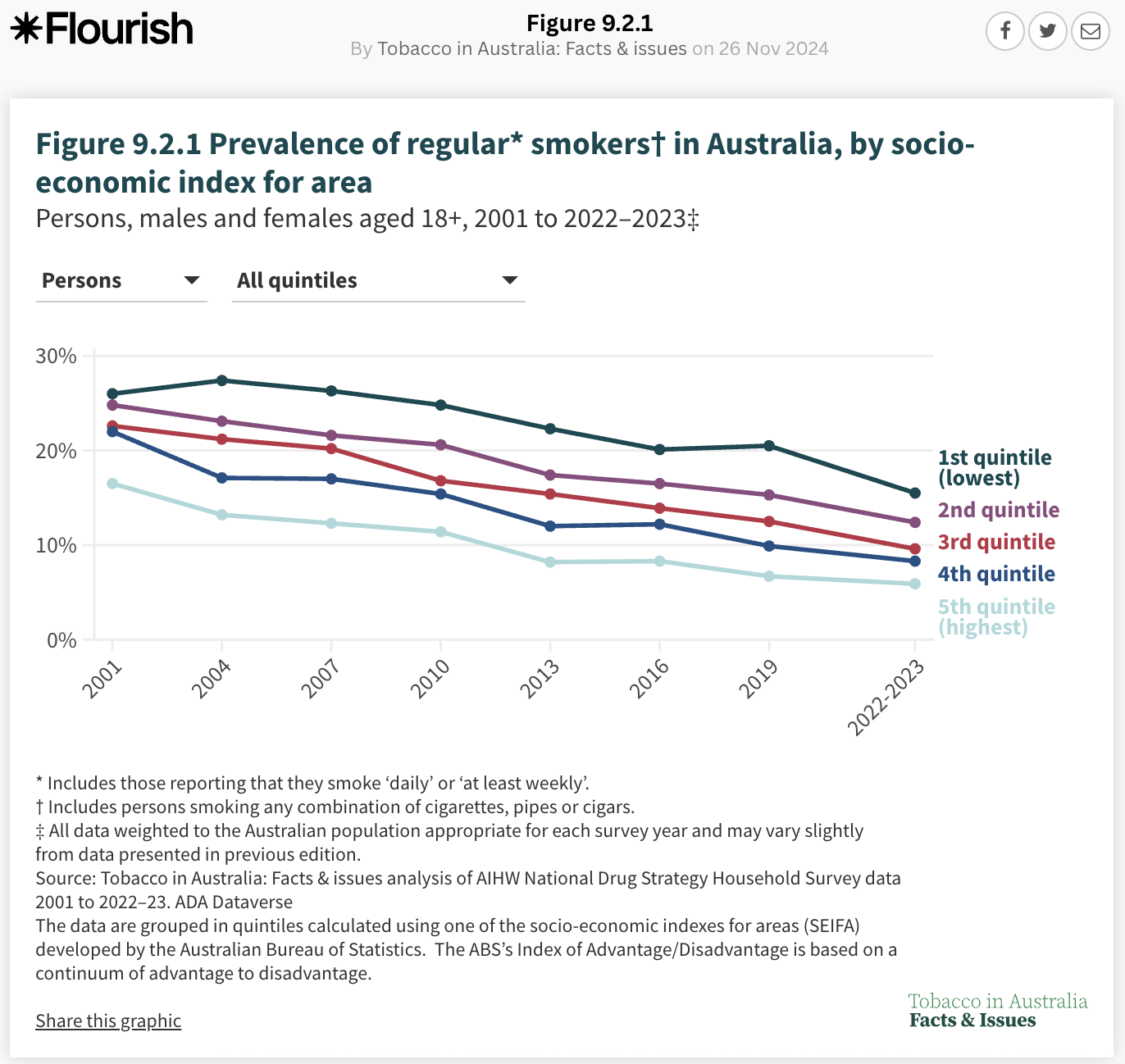
Martin’s claims about tobacco control harming low-income groups are also wildly uninformed. This link could have taken him to oceans of Australian data and graphs showing that, regardless of what definition of disadvantage is used (composite indexes, income, education) disadvantaged Australians have been smoking less in parallel with smoking declines in their more advantaged counterparts, continuously since at least 2001. This is the case for both declining prevalence and reduced cigarettes per day. Here’s just one graph of many that are inconvenient to his argument.
Yes, the lowest levels of disadvantage do have higher smoking rates than those in the highest, but as a criminologist Martin may be ignorant that this observation holds for almost every disease, cause of injury, vital statistic or health related behaviour (diet, obesity, alcohol etc), not just smoking. Poorer health travels with disadvantage.
And more news for him. It is not just tobacco prices which impact those on low incomes more than their more advantaged counterparts. This happens with every good and service they purchase, a truism in every country in the world where there is not perfect income equality for all people. In other words, everywhere.
In Australia today, there are only two groups where a majority of people smoke: those with psychosis and those in prison. In every other group, early school leavers, the unemployed, single parents and First Nations people there are more ex-smokers than smokers. Talk of people who, as Martin insists “can’t or won’t stop” smoking, will always struggle to explain why so many millions of these disadvantaged smokers over the years have managed to quit despite their disadvantage.
They regret having started to smoke, have agency to quit (mostly unaided), and are doing so more and more. Their higher smoking rates are explained far more by decades of higher smoking uptake than by lower quitting rates.
Few laws ever eliminate the problems they were intended to reduce. But we don’t see Martin’s equivalents in road safety calling for reduced penalties for drink driving because they badly sting those on low incomes, or ditching these laws because many continue to be detected over the limit.
We balance the harms to offenders with the declines in road deaths and injuries.
Can there be anything more perverse in public health than believing the poor would benefit by access to cheap cigarettes which will kill two in three long term users?
Cherry picking in Sweden
Sweden has a low smoking rate (4.8%) and according to Martin, this is all down to the enlightened widespread use of non-combustible nicotine, especially snus. Ergo, Australia need only look to Sweden for the answer, right? Here, Martin is a champion cherry picker when it comes to advancing his argument. Smokeless tobacco has been freely available in Canada and the US for decades and in both countries, it has low usage despite this open availability. In the USA, 2.6% of adults currently use smokeless tobacco and in Canada, only 0.6% regularly use it.
So do the US and Canada wipe the floor with Australia in reducing smoking given that they both allow open access to smokeless? Ermmm no. In the US, recent use of any combustible tobacco is 12.6% of adults in 2023-24. And Canada? In 2022 it’s 12.9% for any use in the last 30 days. This compares to 11.1% in Australia in 2022-23. So where’s the dramatic impact in the US and Canada of open access to smokeless tobacco on smoking rates? Why only highlight Sweden?
Sweden was one of the first nations to implement population-wide tobacco control polices like advertising bans, anti-smoking campaigns and health warnings. But clearly there are also cultural reasons why Swedes use smokeless, much in the same way they are unique in taking to surströmming, a famous Swedish fermented herring delicacy. It’s considered one of the world’s most foul-smelling foods, with an overpowering aroma often compared to rotten eggs, sewage and rancid butter. Or like Australians’ passion for vegemite, almost unique in the world.
“Punishing” the tobacco industry
Martin implies that “punishing” the tobacco industry with policies like taxation, plain packaging, and smoking restrictions is somehow a uniquely Australian thing. Is he seriously unaware that the global Framework Convention on Tobacco Control signed by 183 nations, has an entire section (“Article”) devoted to ways of controlling the tobacco industry’s efforts to wreck effective tobacco control? Here’s a report I co-authored for the WHO in 2008, which catalogues the many ways the tobacco industry has sought to defeat, delay, disrupt and dilute effective tobacco control policies. But for Martin, they are apparently now the good guys.
The industry screams loudest about policies that threaten its sales, and the very loudest screams have always been about high tobacco tax. Most people understand what this means, but Martin thinks it’s somehow unseemly and the nice people in Big Tobacco are misunderstood social welfarists leading people away from early deaths.
Here are a few historic examples of the industry screaming about tobacco tax. The tobacco company Philip Morris (Australia) in 1983 said:
… The most certain way to reduce consumption is through price.
… Of all the concerns, there is one – taxation – which alarms us the most. While marketing restrictions and public and passive smoking do depress volume, in our experience taxation depresses it much more severely. Our concern for taxation is, therefore, central to our thinking about smoking and health. It has historically been the area to which we have devoted most resources and for the foreseeable future, I think things will stay that way almost everywhere.
… A high cigarette price, more than any other cigarette attribute, has the most dramatic impact on the share of the quitting population.
In 2011, British American Tobacco’s boss in Australia, David Crow, publicly acknowledged the impact of tobacco tax, telling a Senate committee:
We saw that last year very effectively with the increase in excise. There was a 25% increase in the excise and we saw the volumes go down by about 10.2%; there was about a 10.2% reduction in the industry last year in Australia. (see here at p xviii)
So if these (and many more like them) do not indicate virulent industry concern about tobacco tax, why has it carried on screaming about tax in the same way for at least 43 years?
Reducing tobacco tax?
Martin has been prominent arguing for the “obvious” necessity of reverting tobacco excise tax to the halcyon days before illegal tobacco erupted in Australia. In this he and a handful of others are in lockstep with the entire tobacco industry who have chorused that Australia should revert to 2020 tax levels. The table below shows what this would likely do to recommended retail prices for a current budget brand, JPS.
JPS Classic (20s)
May-20
May-26
Difference
Excise per stick (1)
$0.94964
$1.52829
$0.57865
Excise per pack
$18.99
$30.57
$11.57
Manufacturers cost (2)
$6.65
$8.33
$1.69
Wholesale price per pack of 20 (3)
$25.64
$38.90
$13.26
Retailer margin (4)
$3.72
$4.28
$0.56
GST 1/11th of final price (5)
$2.94
$4.32
$1.38
Final price per pack of 20
Recommended price (listed in wholesale price lists) (3)
$32.30
$47.50
$15.20
(1) ATO tax rates
(2) Manufacturer cost derived by deducting excise from wholesale cost (3) Wholesale & Recommended price lists 2020 and 2026
(4) Retailer margin is at industry discretion
(5) Calculated by dividing the final price by 11
So today, when a pack of illegal cigarettes can be bought for $7 if you buy a carton, in what universe would price sensitive smokers look at a tax-reduced pack of JPS from Woolies for $32.00 and not continue to immediately walk across the street to buy a pack for $7 in an illegal shop –at less than four times the price?
And that $7 price could even go lower. Cambodia is a high corruption index nation (ranking 158/180 worst in the world). It is also a major transit hub for smuggled tobacco to other destinations. There, a pack of locally taxed cigarettes can be bought for as little as 34c. There is clearly wide scope for the price of illegal cigarettes to go much further south if ever required by ever lower tax drops.
And then there’s the inconvenient problem of Martin’s silence on how it happens that there is also massive illicit tobacco trade in many nations with tobacco tax much lower than Australia’s.
Vaping advocates eat, live, breathe and rejoice in their nicotine addiction. But in 2024, they lost the political debate on vaping policy when the Australian Senate voted to make vapes only legally accessible through pharmacies.
You could hear their wailing deep into the night. This heinous decision would make accessing vapes hugely difficult, they swore. It was gently pointed out that Australians make 440m annual visits to some 5000 pharmacies, an average of 18 times per year, walking out with 331m subsidised prescriptions. So onerous that vapers should have to go to such lengths.
They then retorted that the tiny range of allowed flavours were massively unappealing. They’d lost the parliamentary vote, but will never stop insisting that, unlike every inhalable drug in the global pharmacopeia where flavours have never been allowed for safety reasons, it’s just fine with vapes. It’s not OK to inhale flavouring chemicals in lifesaving therapeutics, but it’s quite OK to do that hundreds of times a day when you vape. Makes perfect sense eh?
The two main vaping advocacy groups, the Australian Tobacco Harm Reduction Association (ATHRA) and Legalise Vaping Australia both put up their white flags quietly and shut down. Those remaining are tiny inconsequential echo chambers.
But the recent focus on Australia’s massive illegal tobacco and vape trade has acted like smelling salts to a few punch drunk vaping advocates who were down on the canvas. They are now disporting themselves in new white hero hats holding aloft their messianic vision that the time is now right for the government to repeal its galactic folly on pharmacy-only vape access.
If vapes could be re-liberated from pharmacies and made available through all those highly responsible tobacconists, vape shops and convenience stores (who have never been known to break the law by selling illicit tobacco or selling to kids), many smokers who for the last 12 years have apparently never heard of vapes let alone tried them, would have the tape peeled from their eyes. En masse, they would discard their cheap cigarettes and storm into vape stockists. Smoking prevalence would drop like a stone.
There are a couple of teensy-weensy problems with these wide-eyed fantasies.
First, almost every illegal tobacco shop across the country – and there are thousands — is also stocking illegal vapes and have been doing so for at least four years. The vaping advocates’ dream is already a reality with a huge number of stockists and the cornucopia of flavours they lie awake dreaming of. This being the case, why then haven’t we already seen an avalanche of smokers switching to vapes? Shouldn’t we be seeing vaping going through the roof already?
Not quite.
Second, there are many countries where the very policies that these fantasists dream of are a reality, for many years. Vapes are freely available in much of Europe, across the USA, in Canada, the UK and New Zealand. And sorry to mention this, illegal tobacco also proliferates.
This being the case, it should be obvious that smoking prevalence in such nations should be embarrassing the socks off Australia, right?
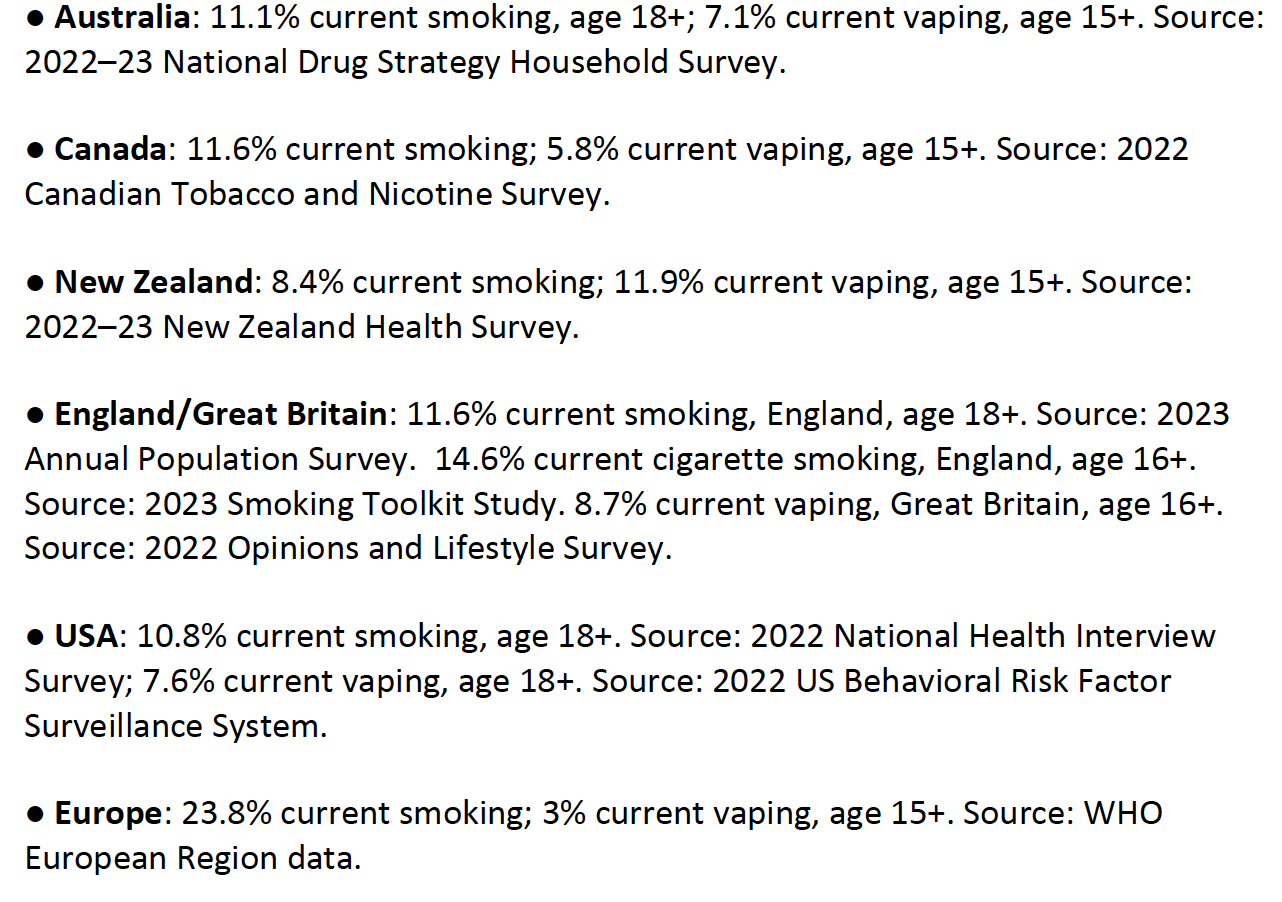
Let’s then take a look at data in a range of countries around the time that Australia’s most recent national data on smoking and vaping was published (the next data will be ready by the end of 2026)
It’s clear that New Zealand is an outlier here: the other comparator regions have similar smoking prevalence, with the Smoking Toolkit Study estimate for England being higher and that for Europe much higher. Similarly striking is Hong Kong: despite banning the sale and public personal possession of vapes, it has just reported a 2025 smoking prevalence of 8.5%, down from 9.1% in 2023.
With highly liberal vape retail access across the past decade occurring as much, if not more, in England, USA and Canada as in New Zealand, and smoking prevalence in all these nations declining, any putative causal generalisation about the downward effect on smoking of liberal versus restricted vape access as in Australia becomes immediately contentious. If liberal access to vaping sees smoking fall across populations, why are not all liberal access nations’ smoking rates much lower than Australia’s after at least a decade of widespread use and liberal access?
And then there’s this bell ringer. In nations where data are available, there are 45 nations which have smoking prevalence under 10%. Just one of these nations (New Zealand) has liberal vape access policy. The rest don’t. So much for the vaping theology that vaping is somehow necessary to reducing smoking to rock bottom.
Other blogs in this series
Vaping theology: 1 The Cancer Council Australia takes huge donations from cigarette retailers. WordPress 30 Jul, 2020
Vaping theology: 2 Tobacco control advocates help Big Tobacco. WordPress 12 Aug, 2020
Vaping theology: 3 Australia’s prescribed vaping model “privileges” Big Tobacco WordPress Feb 15, 2020
Vaping theology: 4 Many in tobacco control do not support open access to vapes because they are just protecting their jobs. WordPress 27 Feb 2021
Vaping theology: 5 I take money from China and Bloomberg to conduct bogus studies. WordPress 6 Mar, 2021
Vaping theology: 6 There’s nicotine in potatoes and tomatoes so should we restrict or ban them too? WordPress 9 Mar, 2021
Vaping theology: 7 Vaping prohibitionists have been punished, hurt, suffered and damaged by Big Tobacco WordPress 2 Jun, 2021
Vaping theology: 9 “Won’t somebody please think of the children”. WordPress 6 Sep, 2021
Vaping theology: 10: Almost all young people who vape regularly are already smokers before they tried vaping. WordPress 10 Sep, 2021
Vaping theology: 11 The sky is about to fall in as nicotine vaping starts to require a prescription in Australia. WordPress 28 Sep, 2021
Vaping theology: 12 Nicotine is not very addictive WordPress 3 Jan 2022
Vaping theology 13: Kids who try vaping and then start smoking,would have started smoking regardless. WordPress 20 Jan, 2023
Vaping theology 14: Policies that strictly regulate vaping will drive huge numbers of vapers back to smoking, causing many deaths. WordPress 13 Feb, 2023
Vaping theology 15: The government’s prescription vape access scheme has failed, so let’s regulate and reward illegal sellers for what they’ve been doing. WordPress 27 Mar 2023
Vaping theology 16: “Humans are not rats, so everybody calm down about nicotine being harmful to teenage brains”. WordPress 13 Jul, 2023
Vaping theology 17: “Vaping advocates need to be civil, polite and respectful” … oh wait. WordPress 3 Oct, 2023
Vaping theology 18: Vaping is a fatally disruptive “Kodak moment” for smoking. WordPress Oct 30, 2023
Vaping theology 19: Vaping explosions are rare and those who mention them are hypocrites. WordPress 17 Nov, 2023
Vaping theology 20 : Today’s smokers are hard core nicotine dependent who’ve tried everything and failed – so they need vapes. WordPress 14 Dec, 2023
Vaping theology 21: Australia’s prescription vapes policy failed and saw rises in underage vaping and smoking. WordPress 10 Jan, 2024
Vaping theology 22: “Prohibition has never worked at any point for any other illicit substance”. WordPress 17 Mar 2024
Vaping theology 23: “84% of the Australian public are opposed to the way the government will regulate vapes” WordPress 2 Apr, 2024
Vaping Theology 24: “Tobacco control advocates are responsible for vape retail store fire bombings and murders. WordPress 27 May, 2024
Vaping theology 25: Vaping is as harmless as breathing in stream. So everyone relax. 10 tenets of vaping harm denial.WordPress 10 Mar, 2026
Not for the first time, NSW Premier Chris Minns has again called for the Albanese government to make significant cuts to tobacco excise tax. He’s now been joined by Nick Coatsworth, someone whose previous contributions to tobacco control policy are elusive. Cutting tobacco tax has now become an established factoid: a prescription repeated so often by lazy journalists who’ve not done the calculations, opposition commentators and callers to radio stations that it is obviously the solution to Australia’s rampant illegal tobacco trade.
Anyone can see, right, that if the price of tax-paid cigarettes could be reduced to make them competitive with untaxed illegal cigarettes, smokers would walk away from the untaxed cheapies and drive them out of the market.
Chris Minns and other politicians in this chorus are used to overseeing multi-billion dollar state financing involving eye-watering elaborate forecasting and modelling. But when it comes to tobacco tax, basic primary school arithmetic appears beyond them.
When those calling for excise reduction move to the next obvious question of the size of their sensible tax cut, a common level proposed is the 2020 rate, a so-called “sweet spot” which preceded the explosion in illegal selling that commenced shortly after. So if we dropped it to there, that would fix the problem, right?
Let’s do the maths.
Australia’s tobacco tax since March 3 this year has been $1.52829 per stick, so $30.57 in tax per pack of 20. In March 2020, excise was $0.94964 or $18.99 per pack. If we take a common fully taxed budget brand now costing $42, this would mean the taxed price would drop by $11.58, the difference between $30.57 and $18.99. So our currently $42 retailed pack would cost $30.42 under this tax-slashed proposal.
Deakin University criminologist James Martin has gone a step further, telling the Singapore Straits Times that Australia should consider ditching tobacco tax altogether. This interesting proposal would place Australia uniquely in the world where no nation or state has zero tobacco tax. Two US tobacco growing states, Kentucky and West Virginia, have very low taxes ($1.10 and $1.20 per pack respectively) and smoking prevalences of 23.6% and 23.8%, levels we’ve not seen in Australia for 35 years.
if the government was to heed Martin’s tax nostrum tomorrow, a typical taxed budget brand costing $42 would then cost $11.43. So would that do the trick and drive illicits out of business?
In Australia, the price today of an illegal, untaxed pack can be as low as $7 if bought by the carton. So a tax drop to 2020 levels would mean a smoker would fork out $30.57, $23.57 or 3.4 times more than they could buy a cheap $7 illegal pack across the road at their nearest illegal tobacconist.
If the government changed Australia’s name to La La Land and axed all tobacco tax, an illegal untaxed $7 pack would still cost $4.43 less per pack than a legal untaxed pack at $11.43.
On either scenario, no budget conscious smoker would ever consider such reductions remotely attractive while illicit cigarettes were still readily available at far less cost.
And let’s remember that a $7 illegal pack includes margins for retailers, transportation from overseas, warehousing and distribution to the retailers, but clearly packs could sell for even less and still remain highly profitable to the criminal syndicates bringing them in.
So how much lower could the illegal price fall? Cambodia is a well-known transit hub for illegal tobacco smuggling. A pack of cigarettes, including local taxes, can be bought there for just 34c. Add margins for illegal retailers, transportation from overseas, warehousing and distribution to the retailers, and there will still be plenty of fat that will allow packs prices to fall far lower than $7.
Globally, there are many examples of nations with very low tobacco tax and very high levels of illicit trade. So if high tobacco tax explains high illicit trade, how is it that so many low taxing countries are awash with black market cigarettes too? Simplistic causal attributions about high tobacco tax clearly hold low generalisable explanatory power about what is a global problem which has often seen the major involvement of established tobacco transnationals.
For decades there have been huge global gaps between official tobacco export and import data. The gaps are explained by large volumes of exports arriving in transit countries where corruption facilitates re-export via illicit trade without any tax being levied.
These penalties, which can also include massive fines and gaol times, are radically changing the risks and costs of engaging in illicit trade in Australia. No country has zero illicit tobacco trade, but those calling for reduced tax are in knowing or gormless lockstep with Big Tobacco which has routinely lobbied government to lower the tax for years to increase their own margins.
Tailpiece #1 John Menadue’s blog, Pearls and Irritations, republished this blog here on May 19. It caught the eye of the lugubrious vape promoter Dr Alex Wodak who reached into his deep lexicon of nastiness (see an earlier blog here), declaring on his BlueSky feed this garbled rubbish (“rather than argument and big smear” …what???) :
Fresh from a 2025 invited tour of British American Tobacco’s “innovation centre” in Southampton, Wodak recently made a doorstopper submission to the recent Australian Senate Enquiry into illicit tobacco.
Across 21 pages, he helpfully included no less than 17 screenshots from Philip Morris and Altria reports to make his argument that reduced harm products like vapes would lead nations away from smoking, a position identical to that of Big Tobacco companies. You could almost feel the love. Invited study tours of Philip Morris innovation centres can surely not be far off.
Odd then indeed that many nations awash with vaping thanks to liberal access policies have not seen them sweep past Australia’s smoking prevalence rate, as I argued with colleagues here.
Odd then too, that with all the years of all this innovation, British American Tobacco still rakes in 82% of its revenue from combustible tobacco. And no tobacco company – unlike car manfacturers transitioning from fossil fuel powered cars to electric vehicles – has yet to name a date whe they will stop making cigarettes.
Tailpiece #2 On Jun 22, 2026 economist Prof Richard Holden who is the UNSW Vice-Chancellor’s Professor Chief Societal Economist and Director of the Manos Institute for Cognitive Economics wrote in hisFinancial Review column that “a small cut in [tobacco] excise won’t reverse this trend now that the illicit market is entrenched. Marginal changes to relative prices won’t do the trick. We have to shift the entire equilibrium by rewinding the clock to 2016. The way to do this is to cut the excise to zero.”
This was very odd, because in 2016 tobacco excise was 61 cents per stick or $12.20 a pack — certainly not a zero tax time (we’d need to go back to 1901 for that).
So I emailed, asking him:
“If all tax was axed, you could buy a pack of (formerly) taxed cigarettes for just over $11. Right now you can buy an illegal pack for $7 if you buy by the carton (which many do). Do you really think that budget conscious smokers would be happy to pay $4 a pack more? If you look at the prices in supermarkets, competition is seldom more than $1.50/pack between budget brands. But cigarettes sell in Cambodia, a major illicit transit country, for as low as 34c/pack. So criminals have massive wriggle room to drop their local prices here far lower and still remain profitable.”
He replied “In my view, cutting the excise to zero would make legal cigarettes cheaper (in equilibrium) than illicit cigarettes and would thus drive the illicit providers out of the market”. Well that’s easy to say, but how given the large price differential that would still remain, would legal untaxed cigarettes compete with illegal cigarettes?. Trying to understand his reasoning here was why I wrote to him. Simply asserting that it would happen is not good enough if you are trying to make a serious case.
We had further email exchanges in which he avoided addressing my question. When I wrote “Please take a look at what has happened to smoking rates in Australia in the last decade. Prevalence in both adults and kids has never been lower … Australia is on the cusp of ending tobacco use by children” he replied “Consumption is up 40% since 2017. That’s just a fact. How can you say we’re on the cusp of ending smoking?” (I had said that we are on the cusp of ending smoking in children).
I then asked him if he was relying on the recent Australian Bureau of Statistics report on nicotine in wastewater for his 40% statement. I wrote: “Are you talking about wastewater data in saying that? If so, you do realise that wastewater measures nicotine, not “smoking” and that the surge in vaping, its massive nicotine delivery (you can get 10,000- 50,000 puff vapes) has likely hugely distorted the picture. There’s also NRT in wastewater. I later discovered on his X account he had made it plain that he thought the wastewater report measured smoking, not nicotine.
The wastewater report states explicitly “it is not possible to discern whether the rise in per capita consumption [of nicotine] reflects a rise in the number of people consuming tobacco and/or existing smokers consuming more.”
He then parried further, asking “You seriously rely on survey data?” and then “I don’t think this is productive. I wish you the best. Please don’t correspond with me any further.” To which I replied “Come on Richard, have a go. You went out on a public limb and I suspect now know you did not think it through. It’s an obvious question I’ve asked you, so what’s the problem in answering or graciously admitting you made a mistake?”
After he closed down our email interaction, I returned to his X account to get some screen shots of my posts to him for this tailpiece, only to find:
I’d made two posts (now removed by his blocking). One was a link to this blog, politely inviting him to explain why he knew better. The second simply noted that the waste water report measured nicotine, not smoking, and that nicotine included tobacco, vapes and nicotine replacement therapy.
But I was “lecturing” him, not questioning him. I am one of those “so-called anti-smoking advocates”, not a researcher for 50 years across a wide range of public health topics.
I resisted using Spotify for several years because a major area of my musical passions was in world music, and particularly African and thought there would be slim pickings. I had many hundreds of CDs and LPs and gradually began digitising them to play on my iPod (remember those?).
After a while I started realising that a large proportion of my soon-to-be-digitised piles were on Spotify. So why was I bothering the slog of digitising? So I kept those that were hard to get or very special to me and sold off the rest. I then proceeded to look for my world and African albums. So many of them were there too.
I built a list of albums and tracks that I couldn’t find on Spotify, and was able to play them from my account. But other people could not hear them. Each year, my list of “not on Spotify” reduced as entire albums or individual tracks were added.
The list below are those from my playlists which I’ve never found there. Youtube has many of them and I’ve uploaded a few sound files myself. So here we go.
Our three year old grandson’s day care recently sent an email to all parents saying there’d been a case of COVID in a child. A week earlier, our boy had a rough night with a temperature and a cough. Panadol syrup calmed him within 30 minutes. By morning he’d rapidly recovered his normal high energy self.
So when the COVID note arrived, we all wondered whether he might have had undiagnosed COVID the week before when he had a 12 hour elevated temperature. His mum and four of his grandparents had seen a lot of him up close. So we all tested ourselves, with me being the only one testing negative over 3 rapid antigen tests. All but I experienced minor symptoms lasting a day or two.
Day care is a universally acknowledged cesspool of infection. Between our three children (now in their 40s) and their five offspring, we’ve seen croup, RSV, Coxscackie disease (hand, foot and mouth), stomach bugs, ear infections and innumerable episodes of snotty noses, coughing, sneezing bouts and fleeting temperatures. Occasionally these saw trips deep in the night to hospital outpatients (for bad croup) and visits to GPs where rest, comfort and panadol and were prescribed.
This commonplace history, experienced by nearly all parents, teaches us childhood infections are inevitable and that rushing off to a GP each time is both unrealistic and unnecessary. It has long been understood that some early childhood infections can promote normal immunological maturation and preventing atopic disease (eczema, asthma, hay fever).
As adults, we use the same decision tree about our own colds with coughs, congestion, muscular aches, and common gut problems. Experience teaches that these are mostly self-limiting unless they persist or are particularly severe. While we often take a day or two off for a bad cold and cancel crowded and close-up interactions, we don’t push the panic buttons that still hover for many about COVID unless there are signs of deadly serious diseases like sepsis and most notifiable diseases (see NSW list here).
But for some, COVID still remains cloaked in a whole different meaning. If you tell someone you have COVID, the experience is often still redolent with the portent that has surrounded diseases at different historic times like bubonic plague, smallpox, tuberculosis, HIV and ebola. Globally, COVID has killed a conservative 7.1 million and infected 780 million since 2019, so this is pretty understandable.
I am in a retirees’ walking group on Fridays and have played tennis on Sunday morning in the fabled Perpetual Wimbledon Qualifiers competition for over 25 years. Both groups have participants in their 60s and 70s, with three in their early 80s. These age groups are at most risk of serious adverse outcomes from COVID infection. Two in my tennis group have chronic conditions and are understandably acutely concerned to minimise exposure to infection.
I heard about my wife’s positive test result about 3 hours into our Friday walk. No one asked me to leave, but I sensed or imagined some anxiety and so caught a train home at the first opportunity. I tested negative when I arrived home, as I did on the next two mornings. I told my tennis group about my and my wife’s status and one of the immuno-suppressed friends said he did not want to risk exposure, regardless of tennis being an open air, non-contact sport. I decided to step down from the game that Sunday to allow him to play. Three players gave me the thumbs up and thank you emojis.
All this stimulated some brushing up on current COVID data and on government recommendations on vaccination, testing and isolation. Here’s a summary of some of the key parameters:
From 14 Oct 2022 in NSW, it was no longer mandatory, only recommended, to self-isolate if you had COVID nor to report a positive test. Most mandatory COVID regulations were repealed at midnight on 30 Nov, 2022 other than those applying in some health and aged care facilities. Many vaccination mandates for health care workers remain (list here)
In 2022, there were 3,345,187 cases of COVID notified to NSW Health. In 2023, the total number of notified cases fell to 307,076 (9.2% that in 2022). The first 111 days of 2026 have seen 12,226 cases. Extrapolated out to 365 days, this may see 40,263 cases notified for 2026, 1.2% of that notified in the peak year 2022. NSW Health has not published weekly COVID numbers since 20 October 2023. It states today that the best measures of COVID-19 in the community are admissions to hospital and in sewage monitoring. Much of the fall-off in COVID cases reflected the major drop-off in people testing with rapid antigen kits.
As at April, 2024 there had been 24,414 COVID deaths among 11,813,144 national COVID cases with 2.7% in those aged under 60 and 55% in those over 85.
COVID vaccination and previous COVID diagnosis do not reduce the incidence of COVID, but critically, they greatly reduce its severity
Young children are at much lower risk from COVID than older adults. Child care services need not notify cases. Parents and staff “don’t have to self-isolate if [they] have COVID-19, but NSW Health strongly recommend [they] stay home to protect others”.
The dramatic fall in the incidence of COVID is explained by changes in immunity to the virus caused by the hybrid effect of huge numbers having been infected and by mass vaccination. Some 97% of adults have been vaccinated at least once in Australia. In the last 12 months, 1.382m doses of COVID vax were administered in Australia, with 60% of these in those over 65 years, and 30.6% in those over 75. Nearly all of these would be booster shots. The graph below shows the fall off across the years of the pandemic.
Discussing all this with a friend who is an international infectious diseases epidemiologist, he remarked “I wonder how many of those who want to keep far away from anyone with COVID or even those living with someone with it, routinely isolate from others in their house and get themselves tested every time they have cold symptoms, because colds and COVID have a lot in common in their early stages. And do they expect or demand all those they live with to do the same? How does all that work out?”
It’s plain there are some who seem to believe that COVID could be fully eradicated like smallpox, and until that time every precaution should continue to be observed as if serious illness and death were waiting around the next corner
My expert friend’s two clearly rhetorical questions obviate that most of us assume that signs of respiratory issues will be trivial, short-lived and passing. Sneezing is universal with an estimated 95% of people sneezing up to four times a day. Adults typically have 2-3 colds a year, with children having more. If we isolated and informed those around us every time we had a sore throat, congestion with body pains or sneezed a few times, we might well rarely leave the house if our concerns were mirrored in others.
They also make it clear that as always, risk perception is only tenuously built on full comprehension and perspective on actual risk but far more on heuristic shorthand cognitive biases anchored to pre-existing beliefs and concerns. Our contagion-minimising behaviours are also inevitably confounded by uncertainty prior to any formal diagnosis.
If those who cohabit with someone who has COVID but who are asymptomatic and have tested negative should be nonetheless avoided, then how does this ethically parse differently to those who make their own assessment that precursor symptoms of possible COVID should not be tested, and they should go out in the world with a clear conscience?
COVID is far from gone, but for all but those with compromised health because of advanced age and co-morbidities like immunological vulnerability, it has mostly moved into the pantheon of sicknesses that will visit many of us from time to time, mostly with little consequence. Except for the very frail old, where COVID today still takes to the stage with ‘flu as a cause of death when death from some cause would have very probably happened within months anyway.
Since December 2023 NSW Health’s advice on minimising the likelihood of spreading COVID to people at higher risk from the disease includes:
Monitor for symptoms. If you have or develop cold or flu symptoms (runny nose, sore throat, cough, fever), stay home until your symptoms have gone. Wear a mask to protect others if you have symptoms and need to leave home
Maintain physical distancing where possible and get together outdoors or in well-ventilated indoor areas.
Regularly wash your hands
Consider doing a rapid antigen test (RAT) before visiting people at higher risk of severe illness. [my emphasis)
Note here, that the advice emphasises that self-isolation need only occur while symptoms are manifest. This is in spite of NSW Health information elsewhere (dated June 2024) saying that people can still be infectious after symptoms end for up to 10 days and that those with no symptoms can be infectious too.
When we test positive for COVID, we rarely know exactly who we acquired it from. When there are people close to us (family, colleagues friends), the principle of parsimony or Occam’s razor suggests that the simplest explanation is the one most likely. So, yes, our grandson did almost certainly spread it to four in his family. But when a family has an “index case” among them, and with many people positive people today not knowing they are positive and never experiencing any symptoms, it is not sensible to finger someone who has tested positive as the definitive person who brought it into our homes or workplaces.
The most important take home in all this is that if you are in your final decade or two, you would be very sensible to do all you reasonably can to minimise the chances that you will be badly affected if you do get COVID.
As I prepared to end this post this, I read an excellent blog by an old South Australian colleague, epidemiologist Prof Adrian Esterman now 77, on the same topic. It has reliable, prudent information on what older people should do to reduce their chances of being seriously affected by COVID. Please read it.
My other blogs on COVID
⭐ over 500 reads ⭐⭐ over 1000 reads
⭐Should COVID vaccine refusniks now be restricted and fined. WordPress 19 Dec, 2021
⭐⭐The very best of cartoonists against COVID-19. WordPress 21 Aug, 2021
1 in 7 Australians still plan not to vaccinate: time to erode this with tough campaigning. WordPress 4 Aug, 2021
⭐⭐Should those avoiding AstraZeneca vaccination because of the clotting risk also avoid having an anaesthetic? WordPress Jun, 2021
⭐Eight common excuses for not being COVID-19 vaccinated and what you can say that might help. WordPress 27 May, 2021
⭐With the risks of AstraZeneca blood clots being tiny, what explains COVID19 vaccine hesitancy? WordPress 23 May, 2021
A reverse white feather? Let all who are COVID19 vaccinated wear a badge proclaiming and normalising it. WordPress 21 May, 2021
⭐⭐What should we make of 10 nations suspending the AstraZeneca COVID-19 vaccine rollout WordPress 15 Mar, 2021
Mandating masks rapidly and dramatically increases mask use: before law 7%, after 97%. WordPress 4 Feb 2021
COVID-19 mask laws drove use through the roof. So where are the data we should megaphone across the world? WordPress 2 Feb, 2021
⭐What’s to be done about Van Morrison and Eric Clapton’s anti-lockdown antics? WordPress 19 Jan, 2021.
Imagine a surgeon refusing to wear a mask. Gladys’ refusal to mandate public masks is this writ large WordPress 21 Dec, 2020
⭐⭐What Dr Fauci didn’t write about COVID19, but well could have. WordPress 14 Sep 2020
When COVID-19 pandemic gets tough the conference scammers get going. WordPress 25 April, 2020
⭐⭐Indelibly sear this into the national public and political DNA: evidence-based prevention saves many lives so let’s honour our COVID-19 heroes. WordPress Apr 22, 2020
⭐⭐How can we erode self-exempting beliefs about COVID-19 contagion and isolation that might subvert flattening the curve. WordPress Apr 19, 2020.
⭐⭐Home isolation: except for food, medicine and exercise. So why are so many other stores open? WordPress Apr 7, 2020
⭐If self-isolating COVID-19 cases won’t isolate, should they be monitored with GPS wearables? WordPress Mar 10, 2020
The total ban on tobacco advertising took a staggering 31 years, from the first bans on smoking in buses, trains and cinemas introduced by NSW transport minister Peter Cox in 1976, through to bans on indoor workplace smoking in the 1980s, on domestic airlines in 1987, in restaurants in time for the 2000 Olympics, and in the last bastions — pubs and clubs — from July 1 2007 – nearly 19 years ago.
Once the first smoking ban was implemented, there could be no turning back: if breathing other people’s smoke was harmful on a city bus or train, by what tortured logic could it be safe on an intercity train or plane, or breathing it in across a whole workday in an office? The pub test failed every time it was asked.
The longest and hardest fought bans here came with those in pubs and clubs, Bar staff, arguably the most exposed of all occupations to tobacco smoke, were apparently unlike every other indoor occupation who were protected by smoking bans. This was always going to be indefensible.
The pub and club industry fed us the hilarious compromise for a few years that smoking was banned within a few metres of a bar, but allowed elsewhere. But somebody forgot to tell the smoke to stay put. Cartoonists had a field day. We saw high-powered exhaust fans proposed that threatened to suck your beer out of the glass; arguments about the birthright of decent Australians to have a smoke with their beer and pie after a hard day’s work (but harming bar staff’s lungs was presumably quite Australian); and as with advertising bans ruining sport and TV profits, endless screaming about economic catasptrophe if you couldn’t smoke in a pub.
Of course, none of this came to pass. Television has not had direct tobacco advertisng revenue since 1976 and smoking has not been allowed in restaurants for 26 years.
When the casino at Barangaroo in Sydney was being built, the O’Farrell Liberal government announced that high roller rooms would be exempt from the smoking ban. I wrote this piece for the Sydney Morning Herald where I sarcastically suggested the government must have obtained research showing that smoke from wealthy high-end gamblers was non-toxic to others. This craziness ended in 2022.
With advertising bans, ads on TV ad radio were the first to go in September 1976 because — as is now being implicitly argued with gambling ads– children watch TV and listen to the radio and would be exposed and stimulated to smoke. But the very same children who saw the very same tobacco ads on billboards, in cinemas, promoting music events or at sporting events were protected by some magic barrier that prevented the ads influencing then there.
Everyone knew this was complete bovine excrement. You can’t be half pregnant so, if ads could influence kids on radio and TV, they obviously could do so anywhere else they saw them. Which was just about everywhere. Politicians had baited their own future traps by conceding ads influenced kids. It was then only a matter of time
So let’s look at the proposed gambling ad reforms
Gambling ads will be banned during live sports broadcasts between 6 am and 8:30 pm, with a limit of three ads per hour outside of play
So it’s OK, yes, for kids staying up late or rising early to watch telecasts of the World Cup football, the Olympics etc and see lots of the same ads that won’t be run in the restricted times? And this never happens. And where’s the data that show up to three ads is benign, while any more are persuasive?
Ads will be prohibited from being targeted at children and cannot be broadcast on radio during school drop-off/pick-up times (8-9 am and 3-4 pm).
But radio ads in the school holidays, all weekend and outside these time on weekdays are all just fine? It’s just those deadly influential ones they might hear on the car radio? And any first year cadet in an advertising agency could argue the case that ads shown to appeal to kids were nonetheless not targeted at them. With this truly pathetic provision, the government has learned nothing from the banning of Paul Hogan from Winfield ads in 1980, when Rothmans tried and failed to use this very reasoning.
Online gambling ads will be restricted to users over 18, and platforms must offer an opt-out mechanism.
This is a notorious quagmire, as we have seen with many reports of under 16s in Australia being able to use VPN workarounds to access social media they are banned from accessing. And critically here, opt out policies are loved by advertisers, because the alternative (opt in) produce drastically lower traffic. The gambling companies could not believe their luck with this inclusion.
Ads must not feature celebrities or professional athletes, and they must include responsible gambling messaging, such as “What’s gambling really costing you?”
Where are these highly fluid class of “celebrities” defined? Will it include the hundreds of vapid come-and-go “influencers”? And what about former athletes? Any suburban solicitor could drive a tank through these porous descriptors.
Australian Labor governments have had strong, world leading appetites for bold tobacco control policy and stood up to powerful industry opposition. Think plain packaging and pharmacy access to vapes. Three in four Australians want gambling ads stopped. This is much higher than support for the 2017 marriage equality plebiscite (61.6%) and even higher than support for more investment in renewable energy (70%).
Banning all gambling advertising would be highly supported by Australians.