It seems that Dr Alex Wodak doesn’t like the Cancer Council Australia very much. Along with the agencies, authorities and government departments all shown below, the Cancer Council supports strong regulation of ecigarettes in Australia, including health minister Greg Hunt’s plan to enforce the current ban on open retail sale of nicotine containing e-juice by making it only available on prescription from 2021. This sets them apart from ATHRA who want to see ecigarettes available as widely as possible, with some advertising allowed, lots of flavours (regardless of whether these appeal to children), and vaping allowed in smokefree areas.

Wodak is one of three directors of ATHRA (Australian Tobacco Harm Reduction Association). ATHRA appears to have no members but accepts donations from supporters. We don’t know how many supporters there are, or how supportive they are. But in 2019 it sought to raise $15,000 but raised only $1,345 from 38 people, falling 88% short of its modest target.
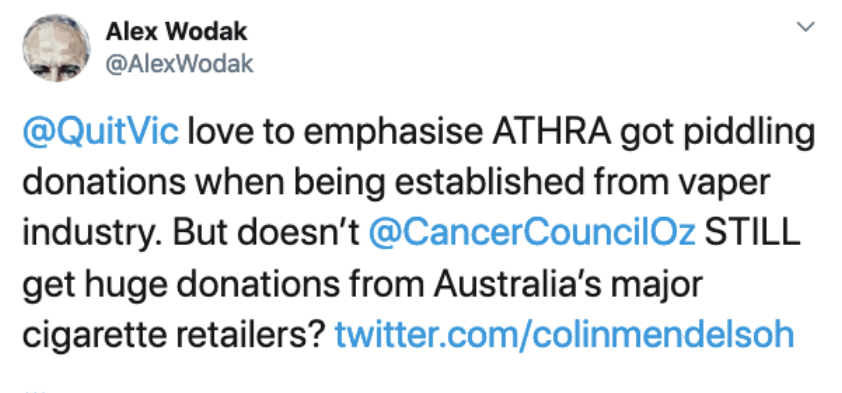
However, in Wodak’s description, ATHRA received two “piddling” donations from two vaping companies at establishment in 2017 totaling $17,500.
ATHRA also received another presumably equally piddling $8,000 “unconditional” support from KAC (Knowledge Action Change), a private British agency. KAC is awash with millions in funding from the Foundation for a Smoke-free World, the “fully independent” agency that happens to be solely funded by Philip Morris International. (KAC has also previously received grants from British American Tobacco’s offshoot Nicoventures.)
If Wodak thinks these donations were piddling, I wonder how he describes the rather more modest donations ATHRA gets from its supporters?
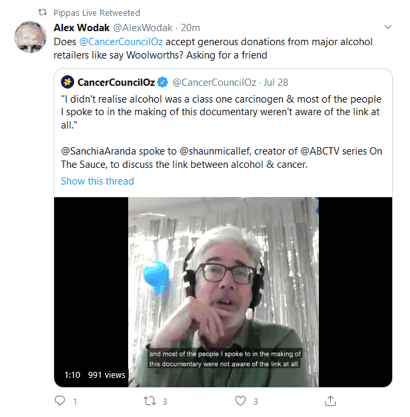
Perhaps smarting at journalists who frequently (and appropriately) question potential commercial influences on ATHRA’s policy positions, Wodak has been busy claiming on Twitter that the Cancer Council takes “HUGE donations from major national retailers of cigarettes”. He also retweeted this claim that Woolworths alone had donated $2m. In fact, he has tweeted references to the Cancer Council takes money from tobacco and alcohol retailers six times in the last nine days.

These allegations of outrageous hypocrisy (“double standards”) sounded extraordinary to me. So I asked the Cancer Council if this was true. Here’s what they told me. All supermarkets except Aldi sell cigarettes, but the funding the Cancer Council received in the past from these chains has not been given by the supermarkets as a slice of their income that included tobacco sales. Instead it has been from in-store fundraising collections and the sale of Cancer Council fundraising daffodil pins, supermarket staff donations, the use of in-store community benefit shopping cards and the sale of Cancer Council sunscreen. All of these sources of fund raising have absolutely nothing to do with tobacco sales, as Wodak implies.
They wrote:
“Cancer Council does not take money directly from industries associated with carcinogen production including the tobacco and alcohol industries. We also avoid any donations that might imply or seem to pressure Cancer Council into adopting policy positions in their favour, such as the pharmaceutical industry, as we value our independent voice on health matters. Cancer Council, like most charities, has accepted fundraising via supermarket networks. In Coles, for example, collections bins for Daffodil Day have raised donations from the public but these donations do not come directly from the supermarkets.”
In 2009 Ritchies IGA supermarkets also donated $1.4m provided by its customers via its Ritchies Community Benefit Card charity initiative.
Perhaps though, Wodak is alluding to some impurity of association in these donations? Is he arguing that the mere fact that the supermarkets, with their hands dirty from selling cigarettes, have metaphorically handled the money obtained from in-store collection boxes or pin sales, making these transfers dirty tobacco money?
If so, every time that he or I or anyone buys anything at a supermarket or fill our cars with fuel from Caltex (Woolworths) or Shell (Coles) or buy liquor from Dan Murphy’s or BWS (Woolworths) or Liquorland, Vintage Cellars or First Choice (Coles) are we also somehow soiled with tobacco associations?
By the same logic Wodak uses here, there is no person in Australia who is not in receipt of benefits partly paid for by tobacco sales. The Commonwealth’s estimate of tobacco excise receipts for 2020-21 is $15.61 billion. This represents 3.2% of expected total government revenue of $490.036 billion. Tobacco tax goes into consolidated revenue along with all government revenue which is used to pay for government expenditure. So every time we all drive on a public road, use a public hospital, send our kids to school, or use any government funded infrastructure, a portion of the cost of those goods and services is funded by smoking. When we get a Medicare rebate payment of say $50, it might even be said that $1.60 of each transfer into our bank comes from tobacco sales.
It does not follow from this that we should all cry and tear out our hair in a moral heap that we are all getting tobacco money. Tobacco tax of course is known to be a powerful factor in driving tobacco consumption down. This 2019 Treasury paper shows (below) the recent historical relationship between excise going up and cigarette sales going down. Because of that, I’m more than fine with tobacco tax: it drives consumption down and provides money for essential infrastructure and government expenditure, as it does in every country.

All this is of course far different to an organisation taking funding directly from vaping companies, or from a third party which distributes money from an agency which receives it all from a tobacco company. Which is what ATHRA has done.
Wodak spent most of his career employed in drug and alcohol services at Sydney’s St Vincent’s Hospital. St Vincent’s Health Australia operates the health and hospital services of the Roman Catholic Sisters of Charity and is part of Mary Aikenhead Ministries. The Catholic church in Australia and globally has of course been the focus of enormous criticism for its record with paedophile priests, for its policies and practices on contraception, abortion, opposition to same-sex marriage and the ordination of women.
On the assumption that Wodak shares the concerns that many have about the Catholic church’s problems, would anyone seriously argue that he therefore had “double standards” in working for a hospital connected with the church, even though the hospital’s drug and alcohol services have nothing to do with any of those policies?
ATHRA’s objectives are anti-smoking as well as pro-vaping (although you will search for a long time before finding any supportive contribution to anything but vaping on their website). I may have missed it (although I don’t think I have), but I’ve not seen ATHRA nor Wodak shaming other charities that the major tobacco supermarket retailers support and calling them out for being in receipt of retail tobacco sourced donations. These include OzHarvest, Foodbank, White Ribbon, Redkite, Children’s Hospitals, Ovarian Cancer Australia, Hummingbird House to name a few. Would a little consistency be too much to ask for?
Wodak has often called for civility in the debate about ecigarettes. Vaping advocates have been frequently far more than odious in all this (see this large collection). If he is sincere in this, he should stop and retract his ill-informed and reputationally damaging accusations about the Cancer Council.
The Cancer Council has a very strong reputation with the Australian public as measured by the 2019 Charity Reputation Tracker scoring over 80%. Cancer Council is the most loved brand in the general charity category measured by Kantar and is also highest in terms of trust by the public. The Cancer Council consistently scores in the top three most trusted charities in Australia in the annual Reader’s Digest Awards alongside Guide Dogs Australia and the RSPCA.

I have seen tweets where vapers have talked about urging people to not donate to the Cancer Council. There is apparently no evidence that this is happening but the consequences of reductions in community support for the amazing work that the Cancer Council has done for many decades in prevention, research and patient support would be frankly appalling.

Tailpiece: one month after this blog was published, Wodak was back on his sad, deflated case, replying to a tweet from someone making another easily checked false statement that “the government” provides most of the Cancer Council’s funding. It doesn’t. It comes from community donations. Plus ça change, plus c’est la même chose.

Declaration: I was an honorary board member of the Cancer Council NSW from 1997-2006
[Edit]
Other blogs in this series
Vaping theology: 1 The Cancer Council Australia takes huge donations from
cigarette retailers. WordPress 30 Jul, 2020
Vaping theology: 2 Tobacco control advocates help Big Tobacco. WordPress 12 Aug, 2020
Vaping theology: 3 Australia’s prescribed vaping model “privileges” Big Tobacco WordPress Feb 15, 2020
Vaping theology: 4 Many in tobacco control do not support open access to vapes because they are just protecting their jobs. WordPress 27 Feb 2021
Vaping theology: 5 I take money from China and Bloomberg to conduct bogus studies. WordPress 6 Mar, 2021
Vaping theology: 6 There’s nicotine in potatoes and tomatoes so should we restrict or ban them too? WordPress 9 Mar, 2021
Vaping theology: 7 Vaping prohibitionists have been punished, hurt, suffered and damaged by Big Tobacco WordPress 2 Jun, 2021
Vaping theology: 8 I hide behind troll account. WordPress 29 Jun, 2021
Vaping theology: 9 “Won’t somebody please think of the children”. WordPress 6 Sep, 2021
Vaping theology: 10: Almost all young people who vape regularly are already smokers before they tried vaping. WordPress 10 Sep, 2021
Vaping theology: 11 The sky is about to fall in as nicotine vaping starts to require a prescription in Australia. WordPress 28 Sep, 2021
Vaping theology: 12 Nicotine is not very addictive WordPress 3 Jan 2022
Vaping theology 13: Kids who try vaping and then start smoking,would have started smoking regardless. WordPress 20 Jan, 2023
Vaping theology 14: Policies that strictly regulate vaping will drive huge
numbers of vapers back to smoking, causing many deaths. WordPress 13 Feb, 2023
Vaping theology 15: The government’s prescription vape access scheme has failed, so let’s regulate and reward illegal sellers for what they’ve been doing. WordPress 27 Mar 2023
Vaping theology 16: “Humans are not rats, so everybody calm down about nicotine being harmful to teenage brains”. WordPress 13 Jul, 2023
Vaping theology 17: “Vaping advocates need to be civil, polite and respectful” … oh wait. WordPress 3 Oct, 2023
Vaping theology 18: Vaping is a fatally disruptive “Kodak moment” for smoking. WordPress Oct 30, 2023
Vaping theology 19: Vaping explosions are rare and those who mention them are hypocrites. WordPress 17 Nov, 2023
Vaping theology 20 : Today’s smokers are hard core nicotine dependent who’ve tried everything and failed – so they need vapes. WordPress 14 Dec, 2023
Vaping theology 21: Australia’s prescription vapes policy failed and saw rises in underage vaping and smoking. WordPress 10 Jan, 2024
Vaping theology 22: “Prohibition has never worked at any point for any other illicit substance”. WordPress 17 Mar 2024
Vaping theology 23: “84% of the Australian public are opposed to the way the government will regulate vapes” WordPress 2 Apr, 2024
Vaping Theology 24: “Tobacco control advocates are responsible for vape retail store fire bombings and murders. WordPress 27 May, 2024