
A couple weeks ago, Oregon haematologist-oncologist, patient advocate and author of Malignant: How Bad Policy and Bad Evidence Harm People with Cancer Vinay Prasad tweeted this

His thread continued: “No physician would dare shame a person who died of lung cancer by sharing a photo of that person smoking in an effort to curb cigarette use It would be despicable, loathsome, & worse; no matter the ‘cautionary lesson’ and yet somehow this idea has vanished for covid19”
And then:
“I understand many are anxious or concerned, and many believe a variety of interventions make sense. But please, doctors do not blame our patients for disease. And, don’t reply to this thread saying ‘this is different’”
Sixteen responded, nearly all agreeing with his views, including some who used his tweet to pile-on the World Health Organization for not having recommended masks earlier than they did.
I posted this in response:
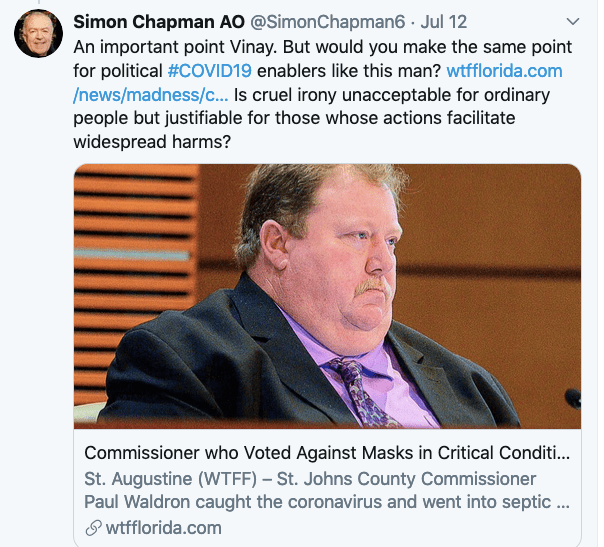
Prasad never responded to me nor to any others. So a few days later I tried again:

Again, no reply. So let’s explore the issues that his tweet raised for me. The argument that a person dead or dying from any disease or trauma should not be shamed or blamed for being a victim of that disease or injury has some obvious ethical and humane merits. But those merits can be parsed.
We rarely if ever see instances of blaming or shaming when the disease involved has important genetic components, when there is an absence of accepted modifiable risk factors for a disease (eg: brain, ovarian, pancreatic cancer), when in the case of traumatic injury deaths, the victim played no part in causing the injurious event, or when the cause of death multi-factorial, with a constellation of contributory issues.
We often though, see comments about the blood alcohol level of someone killed in a motor vehicle, or that someone was not wearing a seat belt. I wrote this piece about the death of Joe Cocker, a heavy smoker, at the age of 70, writing “Confused calls for a cone of “respectful” silence about smoking’s role in cancer and other tobacco-caused disease and for euphemisms about deaths following ‘a long illness’ are forged by the same mentality that thinks tobacco packs should not have graphic health warnings because they might remind people too well about what smoking can do.”
Prasad’s message was directed at his fellow doctors. It was also stimulated by something another doctor had written about someone. If he meant it to apply to all of us as well, he didn’t say so. But it’s worth considering whether the ethical standard he argues for doctors should be any different for all.
His invocation of decency and compassion as reasons for physicians never shaming those who have died go to the widely understood values that it is wrong to speak ill of the dead or to suggest that they had any agency in their fate. The memory of the dead, particularly for those who knew and loved them, should never be desecrated by attempts at shaming them with considerations that they contributed to their own demise. Irony about a person getting their comeuppance from something that in life they went out of their way to avoid, embrace or proclaim drags in widely invoked metaphors about fools’ errands, tempting fate, hubris and the fall of Icarus for flying too near the sun.
The dead are beyond being harmed by shaming or black humour about them “getting what was coming to them”, but those grieving them are blameless and so we show compassion for their loss and not speak ill of the dead. The idea that those who make the effort to shame the dead are “dancing on their graves” in callous disregard for their loved ones’ grief adds a further dimension to the indecency here.
There is also a further consideration. There are very few causes of death which do not display an inverse socioeconomic gradient: the lower the socioeconomic status, the higher the incidence of disease and deaths. Analysts of this have long agreed that this is explained by social, economic and educational disadvantage. If you are little educated and poor, there will be many choices you cannot make as easily as those who are better educated and can afford many options in diet, housing, transport and occupation.
So if those less educated make more unhealthy and dangerous lifestyle choices, much of this can be explained as a consequence of intergenerational poverty and disadvantage. If most people in their families smoke and eat poor diets, an individual growing up in such an environment lives through more unhealthy influences than wealthier, more educated people. If they have little understanding of how to assess quack claims or rubbish being promoted about health risks, they may be far more likely to suffer the consequences. Shaming people in such circumstances can be deplorable victim blaming.
So the ethical imperative to leave the dead in peace enjoys widespread support, particularly when those who died are ordinary, little or unknown people. Those seeking to use their ill fate to advance various public health messages, are seen as vulture-like, runs the argument.
Is it different if you are a public figure who megaphones dangerous nonsense?
But as I read Prasad’s tweet, I immediately thought of many instances of powerful and prominent people who have made pernicious, life-endangering contributions to public health. All of these people have faced widespread incendiary criticism whenever they megaphoned their dangerous and irresponsible views. Think of anti-vaccinationists, politicians enabling the tobacco, fossil fuel, gambling and alcohol industries. Think of those actively trivialising COVID-19 risk, opposing social distancing policies and masks. There is a very long list of such people who have used their prominence in these ways, often undermining public trust in science, thwarting policy and legislation that could save uncountable lives.
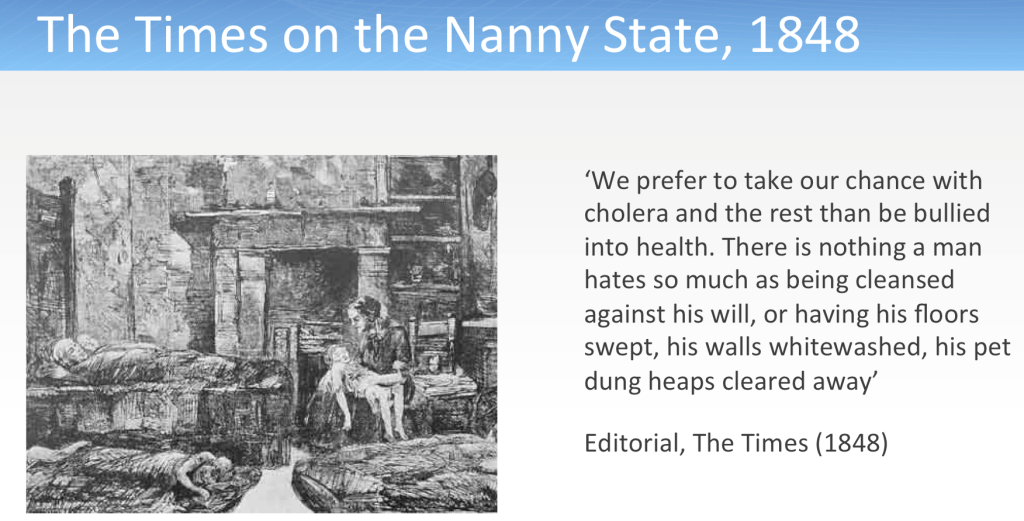
Just as anopheles mosquitoes are vectors for malaria, it has long been argued that the corporations and senior executives of tobacco companies are vectors for the diseases caused by smoking predicted to kill a billion people this century. Those currently aggressively opposing the mandatory wearing of masks in crowded areas are today’s equivalents to the editorial writer at The Times in London in 1848 who fulminated against public hygiene efforts to prevent the spread of cholera
My question to Prasad was whether we should extend the same compassion to influential public figures who might suffer cruel ironies as we would to some unknown individual such as the young person that stimulated his tweet. Brazil’s president Bolsonaro reportedly mocked mask wearing with the homophobic slur that they were “for fairies” prior to acquiring COVID-19 himself. Would Prasad argue that these two facts should go unremarked out of a sense of decency for Bolsonaro and his family?
Brazil has had 2,348,200 COVID-19 cases with 85,385 deaths. It ranks second worst in the world for total cases numbers after the USA. Is it unethical to use Bolsonaro’s illness to highlight cases of people like Bolsonaro as COVOD-19 super spreaders because of their policies and statements like the one above, or should doctors (and everyone) stifle any criticism of him because he has acquired the deadly disease his policies have enabled the spread of and is thereby off limits?
I’m in no doubt that in such cases, the power of cruel irony can instantly and powerfully be penny-drop moments in public understanding. This in turn might play a role in (here) accelerating mask adoption and social distancing, self-evidently good things.
In 1982, the late Nigel Gray AO, a pioneer of Australian and global tobacco control, told two tobacco industry executives on national Australian television “I actually think that the responsible policy makers in the tobacco industry should smoke a lot. I think that would be good for society.” (the link shows him making that statement)
This was both an amazingly cruel but also powerful way of pointing to a core hypocrisy that abounds in the tobacco industry where many senior employees and directors do not smoke but spend their days devising promotions and appeals to get as many people as possible to do so. Doubtless they would argue that they choose not to smoke. While the male head of a lingerie company would not be expected to “choose” to wear women’s underwear, smoking is a choice open to all. It is scarcely imaginable that the chairman of Ford would drive a Toyota or the head of the Meat Marketing Board would be a vegetarian. Such lack of personal confidence in their products would probably see them not long in their jobs. The tobacco industry does not seem to mind such an irony.
As Nigel Gray did in that interview, there are times when we should rub the faces of such people in these ironies.
