I have a dear friend who has lived with strong pain every day and night for over a decade. Following extensive damage to her spine from osteoporosis, she was advised to have a spinal fusion operation, on threat of needing a wheelchair for the rest of her life. She has a metal “cage” supporting her lower spine but pain fills her life. More often than not, she wakes several times a night and gets some relief from hot showers. Pain relieving drugs are a daily part of her life. Globally, millions of people live with unremitting pain. If you are in pain, it dominates your life.
I originally published this piece (below) in the Sydney Morning Herald, 18 September, 1999. It was republished in a collection of 71 of my writings on health Smoke Signals, in 2016.
In 1809, 47 year old Jane Crawford risked scalping and the tomahawk to ride her horse 60 miles in four days to the practice of Dr Ephraim McDowell in Danville, Kentucky. Mrs Crawford’s ovarian tumour was giving her unremitting, labour like pain. While several men held her arms and legs, and she recited psalms, McDowell took 25 minutes to cut a 14cm incision in her lower belly, remove a 1.2kg tumour and then sew her up with interrupted sutures. Outside the house, an angry and incredulous mob not unlike those who would today seek to close heroin injecting rooms that minister to a different sort of pain, waited ready to lynch McDowell should his patient die. Five days later she was out of bed and lived for another thirty years.
McDowell’s pioneering operation and his patient’s courage are historical landmarks in the annals of surgery.
While opium and cocaine have been used since antiquity for pain relief, it was not until 1846 when Thomas Morton first used ether to anaesthetise a patient for a tooth extraction that lengthy and detailed surgery more subtle than crude hacking could be performed under general anaesthesia. The next year, chloroform was used for the first time to relieve pain in childbirth and went on to become the anaesthetic of choice for more than a century. Today, pain management specialists estimate that more than 90% of postsurgical, post-trauma and cancer pain can be fully relieved, and 75% in chronic, non-cancer pain such as arthritis. Thirty years ago, these figures hovered around 10%. Worldwide though, only half those suffering from these conditions have access to services and drugs which can provide this relief.
Proust wrote that “Illness is the doctor to whom we pay most heed: to kindness, to knowledge we make promises only; pain we obey.” People in pain are preoccupied by the experience. Pain bulldozes all emotions aside, including hope. Yet pain produces a bewildering range of ambivalence. While aspirin and paracetamol are the most commonly used drugs, and around one in five experience pain that has lasted longer than three months, so often we conspire to deny the reality of pain. We feel obliged to cheer the injured footballer who returns to the fray after losing teeth or being knocked unconscious. Many couples make a virtue out of refusing pain relief in childbirth. While a woman begs for an epidural, her husband gently counsels “remember we agreed … no drugs”. Many who have lived with pain tell of the scepticism of others (“You don’t look like you’re in pain”) but also of the subtle imperatives to stop their misery infecting those around them. Anglo and Asian women tend to be stoic in childbirth, while southern European and Arabic women are uninhibited in their expression. Moralists, including many in medicine, have often denied the dying sufficient morphine, fretting that they might become addicted.
Recently, television allowed us to consider the abandoned Serbian torture chamber, where unspeakable degradations were wrought on its Kosovar captives. Torture is the active infliction of pain on its unwilling victims. Professor Michael Cousins, head of the Pain Management Research Centre at Sydney’s Royal North Shore Hospital, describes unrelieved pain as “torture by omission”. The United Nations Declaration of Human Rights codifies civilised society’s most basic standards and aspirations for its citizens.
Yet as Cousins points out, the Declaration says nothing about the most elemental concern of all: the right to be relieved from pain.
This remarkable omission is a testimony to our ambivalence about pain. Its consequence is that pain management as a medical speciality lives a Cinderella existence, shining occasionally as islands of enlightenment in a sea of misery. The most recent and exciting developments involve discoveries about the way that damaged nerve endings sprout pain fibres, the growth of which can be inhibited and so the pain controlled through drugs administered through surgically implanted mini pumps. People who have lived for years in desperate pain are now being assisted to live largely pain-free lives again through such developments. Yet there are only seven pain management training centres in Australia, and for all the pious political talk of the need for palliative care after the overturning of the Northern Territory euthanasia legislation, cruelly token budgets have found their way into health expenditure in the period since.
As historically unprecedented falls in fecundity, better living standards and the successes of public health combine to cause the age distribution of the world’s populations to balloon increasingly to the right of the graph, more people will live with the pain of chronic degenerative conditions and cancer. Despite this, the disabling and all-absorbing nature of pain often militates against its victims becoming potent advocates for pain relief to be declared a basic human right, and all that would flow from this. If Cousins’ and his colleagues’ mission were to succeed, what a gift to the world this would be.
I write to draw attention to the pernicious creep of “preventative” instead of “preventive” in what the ABC broadcasts. Your pronunciation standards guide, ABC Pronounce, formally notes that “preventive”, not preventative be used. This ruling has been in place since 1989.
Tonight on the Sydney 7pm news bulletin, the words “preventative medicine” bannered an item on vaping. I’ve noticed it several times recently.
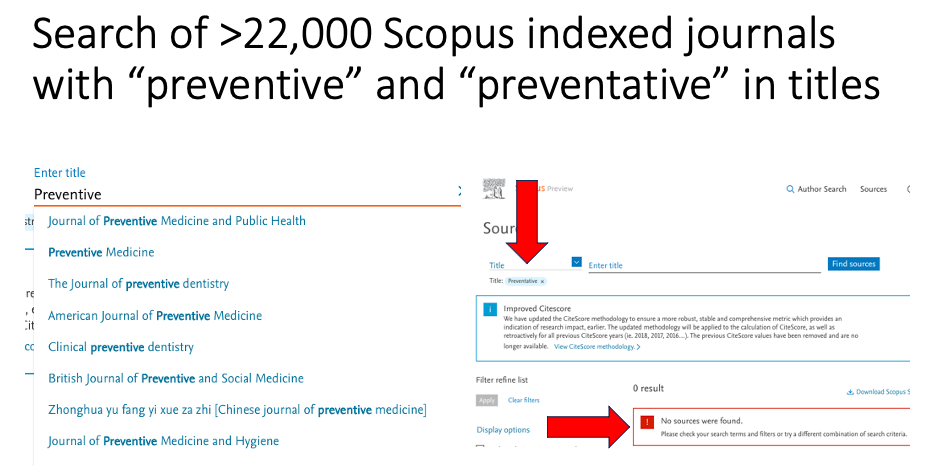
Scopus, the scientific world’s largest and most respected scholarly reference service indexes over 22,000 journals. Not one of these has the word “preventative” in its title, but there are 10 with “preventive” (see https://www.scopus.com/sources.uri)
The School of Public Health at the University of Sydney was the first school of public health in Australia and the first to offer a Masters in Public Health (in 1978). At the time it had a Department of Preventive and Social Medicine. I was on the staff from the first intake of students and today have an emeritus appointment in the School.
Across 45 years, there have been countless times when staff in the School have rolled their eyes and corrected students’ essays and treatises by changing “preventative” to “preventive”. “Preventative” is an infectious Americanism which has attained its currency by brute force of repetition. It grates in the ears of anyone working in this field . I’d put it in the same league as the American pronunciation of “defence” (“dee-fence”). I’ve never heard an American official refer to the US Department of Dee-Fence, yet the dee-word is endemic in sports commentators.
Sorry, but anyone who pairs “preventative” with “medicine” immediately marks themselves as someone who has never actually worked in preventive medicine.
The knock-out argument here is this: there is no verb to “preventate”. We simply prevent things and in public health, preventive medicine is a major division in the discipline of public health.
When the definitive history of tobacco control is written, it will record a most peculiar phenomenon. British tobacco control experts cannot help themselves from schooling Australian colonial numbskulls about where we are going so very wrong with vaping. Britain really has better vaping policy than Australia, they keep telling us.
This is quite amusing because as we’ll see below, some 10 years after the major boom in vaping commenced, vaping prevalence is higher in Britain than in Australia and you could put a cigarette paper between the smoking prevalences of the two countries. And in the last 30 years, Australia has always had the gall to implement nearly every major policy change ahead of Britain. So that’s quite a herd of elephants in the room.
Pro-vaping English researchers and advocates have often written submissions to government enquiries in Australia where they tried to explain England’s superior track record. It’s all a bit like the equivalent of Britain’s fanatical one-eyed Barmy Army cricket supporters who insist that England – not Australia – really won the 2023 Ashes series; that England’s Jonny Bairstow should not have been given out stumped in the 2023 second test at Lords; that England really were the best team at the 2023 One Day World Cup, despite coming seventh below even the Afghanistan minnows while Australia humiliated an apparently invincible India in the final.
This has been going on for some time, Australia and England have met in 361 test matches since 1877. Australia has won 152 and England 112, with 97 ending in draws.
So what about smoking and vaping? With tobacco control, there is almost nothing in recent decades that the Poms had the initiative or mettle to introduce before Australia showed them the way. They have always been the bridesmaids. Here are a few examples:
Graphic health warnings: Australia followed the 2000 lead of Canada in introducing graphic picture health warnings on packs in 2006. Britain implemented them in Oct 2008.
Pub smoking bans: Australian states and territories began banning smoking in pubs from 1998, Britain did it in July 2007
Plain packaging: Australia implemented it Dec 1 2012, the world’s first. Britain: in May 2017.
Smokeless tobacco ban: Australia June 1991; Britain in 1992 (following a EU Tobacco Products Directive)
Price of cigarettes: Australia #1 in the world ($US25.88 a pack); UK #2 ($US15.83 – 39% less)
Retail display bans:NSW got the ball rolling in July 2008, with all states subsequently following. England and Wales: from 26 May 2015.
English apoplexy over Australia’s prescription access to vapes
“[F]irst, rigorous enforcement of the ban on vapes and snus sales to children and young people under 18, with punitive measures for non-compliance; second, ban the sale of snus and vapes to adults except when prescribed for smoking cessation, as, in our experience, wider availability enables them to fall into children’s hands; and third, introduce a total ban on disposable vapes.”
All three measures are central to Australia’s recently announced policy on vaping.
So how did England’s leading tobacco control advocacy group react to this call? Deborah Arnott, chief executive of health charity Action on Smoking and Health (ASH) was quoted in a press report on the paediatricans’ letter as saying: “ASH wants action to curb youth vaping, but making vapes only available on prescription won’t help, after they tried this in Australia underage smoking and vaping both went up … Australia’s aggressive anti-vaping policy opened the door to illegal vapes, conflated the harms of vaping with smoking and left tobacco cigarettes, which are far more harmful, on sale everywhere. ASH supports evidence-based measures to curb youth vaping, by prohibiting branding and marketing appealing to children. The disposable vapes that have surged in popularity in recent years are available for pocket money prices on every street corner and they’re currently packaged more like a sweet or a toy than a smoking cessation device. This is unacceptable and must change.”
So let’s take a look at Arnott’s ignorance of what has actually happened in Australia, and her formidable abilities to walk on both sides of the street at once.
She says Australia “tried this” (ie prescription access to vapes) and then “underage smoking and vaping both went up”.
Predictably, this saw the surviving prescription access component fail to be taken up by nearly all Australian doctors and vapers. Why would smokers bother to go to a doctor to get a script for vapes when they – plus legions of non-smokers including kids who were “recreationally vaping” — could buy vapes easily right across the country?
This failure had nothing to do with the prescription access component, but everything to do with the useful idiots in the far right of politics and their urgers in vaping advocacy who held the national door open for unrestrained illicit trade.
Notably too, all this happened during the COVID pandemic, when state and federal governments seconded thousands of health department hands to be on deck for COVID-related duties. As a result, the requirement that vapes could only be sold to those with a prescription was almost totally ignored by retailers, knowing that its policing was being accorded all but zero priority by health departments. You could buy vapes almost anywhere. Just like you have always been able to do in Britain. Imagine what would have happened if pharmacies decided to ignore the law and sold prescribed drugs to anyone wanting them. Pharmacists would have been struck off, or even jailed.
Arnott appears to have dined out on the huge propaganda campaign designed to discredit the politically gutted prescription policy internationally, straight from the industry’s playbook it tried (and badly failed) to use in stopping the spread of plain packaging legislation
And then she says that Australia shockingly “left cigarettes on sale everywhere” while it attempted to implement prescription access. Ermmm … just like Britain and every other nation in the world has left them on sale everywhere! This is the same old populist knee-jerk reaction we have seen about every significant piece of tobacco control policy “this is window-dressing! If you’re really serious about stopping smoking, why don’t you just ban cigarettes”.
I dealt with the wittering myopia of this argument in an earlier blog. The argument that you cannot seriously regulate vapes (as Australia is now doing) for as long as cigarettes are sold to anyone over 18 would have to be among the most cringeworthy, forelock tugging pieces of defeatism in contemporary public health.
I have often heard public health leaders say “If cigarettes were invented today, and we knew all we know about their dangers that we know now, not a country in the world would allow them to be sold.” Well, Trump’s America might. It took more than half a century of smoking for us to understand the full risks of smoking. Those who run this argument are effectively saying “let’s learn nothing from the history of smoking-caused disease and its control, let’s just let vaping rip like we did with cigarettes and cross our fingers about any down-the-track consequences”.
Restricting access to vapes through prescription allows smokers with serious intent to quit smoking another option. Importantly, a homeopathically small number of doctors would issue children or non-smokers with scripts for vapes, whereas they can access them with ease under Arnott’s preferred policy.
Opponents of prescription access – especially those interests centred on selling vapes to as many people as possible – have megaphoned the alleged “failure” of Australia’s prescription policy. It speaks volumes about the arrogance of English tobacco control, that the head of its oldest advocacy agency is apparently so clueless about what actually happened in Australia.
ASH England supports “adults only” targeted vaping marketing
She continues: “ASH supports evidence-based measures to curb youth vaping, by prohibiting branding and marketing appealing to children.”
This is truly gob-smacking stuff. When I started in tobacco control in the late 1970s, the main challenge was getting rid of tobacco advertising and promotions. The tobacco industry ran the argument on repeat for over a decade that there was such a thing as tobacco advertising that appealed to adults but not to children. We should let that bloom, they argued, but jump on not ads that beguiled kids. Some never-specified, surely magic barrier prevented “adult” advertising messages from ever penetrating the orbits of children. No one in the advertising industry had ever heard of such barriers.
UK legislation on permitted vaping advertising is classic, absurd “half pregnant” policy: ads are banned on radio, television and magazines, but not in cinemas, posters, leaflets or bus sides. The UK Government has been advised that British kids apparently never go to the movies, see billboards or see buses when they pass.
In 2024 Deborah Arnott has climbed in her tardis, inviting us to believe in the same tooth fairy “evidence-based” controls when it comes to neutering vape marketing to kids.
And then we need to ask why, if vaping is as benign to health as its advocates claim it is, do they nonetheless feel bound to say that they want to “curb youth vaping”. Why not treat vaping like yo-yos, hula hoops, fidget spinners and other harmless childhood fads, as a leading pro-vaping Australian advocate once suggested. Seriously.
In Australia in 2022, one in ten (10.6%) adults were current daily smokers. This rate has steadily declined from 22.4% in 2001. This report did not provide data on less than daily current smoking prevalence. However an earlier (different) national survey showed that another 1-2% smoke not daily but less than monthly. So the two countries are about the same.
Vaping In Britain 8.7% of adults currently vape daily or occasionally, an increase from 2021 where 7.7% of people reported daily or occasional e-cigarette use. Vaping is highest among those aged 16 to 24 years in Great Britain; the percentage of people in this age group who were daily or occasional vapers in 2022 has increased to 15.5%, up from 11.1% in 2021.
In Britain in 2023, 20.5% of children 11-17 had tried vaping, up from 15% in 2022 with 7.6% currently vaping, up from 6.9%.
In Australia, there has been a far more dramatic increase between 2017 and 2022/23 in both “ever” vaping and current (past month) vaping in school children aged 12-17. Just under 30% of Australian school students have now tried vaping. The figure below shows a significant fall in exclusive smoking that is in line with the historic trend downward. In 2017 9.7% of students were either exclusively vaping or vaping and smoking (dual using) while in 2022-23 this had shot up to an alarming 16%, more than 1 in 6.
Given that only 7.3% of students were exclusively smoking and/or dual using in 2017, it follows that the lion’s share of the increase in vaping has occurred in children who had never smoked: they had taken up vaping not as a substitute for smoking, with some undoubtedly also then also taking up smoking (longitudinal studies show that children who take up vaping have a three-fold greater probability of later taking up smoking).
As we saw above, Britain has played catch-up with Australia on almost every tobacco control policy. Like Australia, it has seen rapid growth in vaping by children, many of whom have never smoked. And like Australia, it has seen historic falls in smoking by children which long preceded the advent of vapes. Our adult smoking rates are about the same, while Australia’s adult vaping prevalence is half that of Britain’s.
This all raises serious questions about which population groups are being most affected by vaping. Vaping prevalence is rising far more than smoking prevalence is falling. So claims that vaping is a population-wide game changer in smoking cessation are clearly hype. But there is unequivocal evidence that the present arrangements for vaping access are seeing massive rises in kids being exposed to the addictive highly drug nicotine. This is no accident but as central to the vaping industry’s business plan as securing smoking in successive cohorts of teenagers was to the tobacco industry (where today, every company is heavily invested in vapes).
These data underscore the importance of the Australian government’s policies to get vapes out of the reach of kids by making them prescription access only.
Other blogs in this series
Vaping theology: 1 The Cancer Council Australia takes huge donations from cigarette retailers. WordPress 30 Jul, 2020
Vaping theology: 2 Tobacco control advocates help Big Tobacco. WordPress 12 Aug, 2020
Vaping theology: 3 Australia’s prescribed vaping model “privileges” Big Tobacco WordPress Feb 15, 2020
Vaping theology: 4 Many in tobacco control do not support open access to vapes because they are just protecting their jobs. WordPress 27 Feb 2021
Vaping theology: 5 I take money from China and Bloomberg to conduct bogus studies. WordPress 6 Mar, 2021
Vaping theology: 6 There’s nicotine in potatoes and tomatoes so should we restrict or ban them too? WordPress 9 Mar, 2021
Vaping theology: 7 Vaping prohibitionists have been punished, hurt, suffered and damaged by Big Tobacco WordPress 2 Jun, 2021
Vaping theology: 9 “Won’t somebody please think of the children”. WordPress 6 Sep, 2021
Vaping theology: 10: Almost all young people who vape regularly are already smokers before they tried vaping. WordPress 10 Sep, 2021
Vaping theology: 11 The sky is about to fall in as nicotine vaping starts to require a prescription in Australia. WordPress 28 Sep, 2021
Vaping theology: 12 Nicotine is not very addictive WordPress 3 Jan 2022
Vaping theology 13: Kids who try vaping and then start smoking,would have started smoking regardless. WordPress 20 Jan, 2023
Vaping theology 14: Policies that strictly regulate vaping will drive huge numbers of vapers back to smoking, causing many deaths. WordPress 13 Feb, 2023
Vaping theology 15: The government’s prescription vape access scheme has failed, so let’s regulate and reward illegal sellers for what they’ve been doing. WordPress 27 Mar 2023
Vaping theology 16: “Humans are not rats, so everybody calm down about nicotine being harmful to teenage brains”. WordPress 13 Jul, 2023
Vaping theology 17: “Vaping advocates need to be civil, polite and respectful” … oh wait. WordPress 3 Oct, 2023
Vaping theology 18: Vaping is a fatally disruptive “Kodak moment” for smoking. WordPress Oct 30, 2023
Vaping theology 19: Vaping explosions are rare and those who mention them are hypocrites. WordPress 17 Nov, 2023
Vaping theology 20 : Today’s smokers are hard core nicotine dependent who’ve tried everything and failed – so they need vapes. WordPress 14 Dec, 2023
Vaping theology 21: Australia’s prescription vapes policy failed and saw rises in underage vaping and smoking. WordPress 10 Jan, 2024
Vaping theology 22: “Prohibition has never worked at any point for any other illicit substance”. WordPress 17 Mar 2024
Vaping theology 23: “84% of the Australian public are opposed to the way the government will regulate vapes” WordPress 2 Apr, 2024
Vaping Theology 24: “Tobacco control advocates are responsible for vape retail store fire bombings and murders. WordPress 27 May, 2024