Our house is filled with artwork, cloth and knick-knacks we’ve picked up over decades of travel.
I often wonder what I’d take if we chose to downsize to an apartment when zimmer frames make the house too difficult. Here are seven very special pieces that I’ll take to my grave.
Maoist kitsch
I bought this statuette in a Beijing flea market about 20 years ago for $15. These pieces were massively popular during the Maoist cultural revolution in China and now command sometimes high prices from kitsch aficionados.
I took it back securely wrapped in hand luggage where it went to my university office, sitting on my desk for several years.
One day a Chinese student came to see me for feedback on an essay. I saw her look at the figurine and asked her “so who is the man kneeling? Is he someone well known, or is he a particular kind of worker or dissident?” This much seemed obvious.
She looked very awkward and said carefully “It’s no one special … but he’s a professor”
I could not have been more delighted to learn this. Clearly here was someone who might have been me, had I been an academic in Maoist China. The red guard holds aloft Mao’s Little Red Book, the only book worth reading, and stands on his shoulder, publicly humiliating the professor in his re-education.
“So what does the wording on the sign around his neck say?” I asked.
She seemed mortified and looked at the floor. I assured her that I knew it must have been something awful about the professor. She could tell me. I wouldn’t be offended.
After some moments, she sheepishly told me that it said “Academics are parasites on society”.
The fish mouth vase or water jug
This truly bizarre piece was the featured image in the catalogue at a Lawson’s decorative arts and objects auction several years ago. We’ve had a koi pond for 25 years (photo below), and their beauty has since piqued my interest in fish art and objects. So this item burned into my attention. I won the bid and took it home, to my wife’s horror.
It had a dark residue inside suggesting it had been used to keep flowers in water. I cleaned this out and now use it to pour table water at dinners. A single kanji character on the base told a neighbour who is a fine arts specialist that it’s Japanese.
Our koi pond at dusk
Senegalese barbershop advertising sign
I’m an Africaphile and have spent hundreds of hours in the African quarters of cities in record and CD shops when these used to be common. On a trip to New York about 30 years ago, I bought this painting in a small SoHo gallery. I’d seen many of its kind before. They are front-of-shop advertising signs for barber and hairdressing shops in West Africa.
My parents were both hairdressers. They had many magazines in their salon’s waiting area with hundreds of photos of women’s hairstyles that customers could browse for ideas as they waited their turn. So this barbershop art resonated strongly with my childhood.
This one is one of the best examples I’ve seen, among many that are far more naïve in the quality of the art (see large selection here). I have a book in French Ici bon coiffeur by Jean-Marie Lerat (1992) which shows examples from most West African nations.
Beatles drawing
On the same New York trip when I found the barbershop ad, I found this ink drawing being sold by a wizened up old man, selling his work from a square card table on the footpath, again in SoHo. As the Beatles audition, a slovenly record executive asks “What else do you do?” I thought it was perfectly witty and paid something ridiculously small like $20 for it.
I noticed it was signed “Tuli”. In my teens I’d been a huge fan of the New York beat poets rock band The Fugs . Named as a nod to Norman Mailer’s book The naked and the dead where he substituted “fug” for “fuck” to taunt puritanical censorship policies of the time, their most famous song was the salacious Boobs a Lot. I loved the driving Group Grope off their second album too. Country town Simon thought they were just cooler than. Tuli Kupferberg was a core Fugs member.
So I said to him “Are you Tuli Kupferberg, by any chance?” and knock me over, he was! He was delighted to be recognised. We chatted excitedly for 20 minutes or so and he invited me to his place that evening with the promise of illicit experiences. I gave my excuses. He died in 2010 at 86. The sex, drugs and roll n’ roll didn’t cut him short.
Our original Modigliani
Wandering one morning in Ho Chi Minh city years back, we saw a labyrinthine art shop with several artists inside painting portraits from photographs and copies of famous paintings from books.
And then we saw it. A clearly original Amedeo Modigliani. In fact, a painting so famous that it graces the cover of the Taschen collection by Doris Kyrstof (see below). And here it was in front of us, with the shop owner clearly unaware of its immense value. After a lengthy tea ceremony, we shook hands on $40. We’re sending it to Southeby’s next year.
We also bought a Van Gough haystacks original.
Turkish shop dioramas
I’ve been to Turkey several times since the early 1970s. Istanbul should be on every traveller’s bucket list. One day in 2014, walking on the shore of the Bosphorus after a night singing on a marriage boat, I found a small shop selling intricate diaoramas of old Turkish shop fronts. There were many to choose from, all about $120. I bought two and on return visits have bought more. Pictured (top to bottom) are a general grocery shop, a fish monger, a bakery and a fruit and vegetable shop.
These miniatures transport me back to childhood nativity, military and historical diaoramas that fascinated me and which I crudely constructed in shoeboxes with toy soldiers, knights and cowboys.
Reg Mombassa tunes up
When COVID restrictions in Sydney lifted after months of us being cooped up, it was announced that we could have a maximum of 20 people at home, in addition to those living there.
A tennis mate, Dizzy, called me and said that in celebration, he wanted to host a pay-to-come house concert to raise money for a charity in Indigenous housing. His contribution would be to pay for the musos. Did I know how to contact Dog Trumpet? I did, and gave him the details. Pete and Reg jumped at the idea.
So on a Saturday night in Dizzy and Margot’s amazing renovation of the upstairs of a Balmain shop, 20 guests joined them for a two set gig in the living room. Another friend, the photo gallery owner Phillip Bell came along too. He took the stunning photo below and sold it to me at mate’s rates.
I always think of Vermeer when I take it in.
The central bottom right window pane, you can see Reg Mombassa tuning up before the start. Everyone was mesmerised by their sheer, original talent and easy presence throughout the best of nights. If you don’t know their work, here are two of my favourite pieces. Buttons undone and Bored wife.
The report of the Senate Inquiry into the regulation of vapes has been published. It will inform the debate in the Senate scheduled for the June sitting.
The Greens will play a pivotal role in the outcome of the vote. In the report, their concerns are well expressed – particularly when it comes to the detail of how we can be assured that possession of vapes is not criminalised – only commercial supply and sales outside of that which will be dispensed to those with prescriptions will be hit with huge deterrent fines. No one. No one wants users to be prosecuted, fined or otherwise criminalised. The only exception should be where people ignore no smoking or vaping regulations, as has long been the case with smoking. Every airline in the world bans vaping.
The Bill does not ban or prohibit vapes
But the Greens are apparently exercised about “prohibition”. As a section of the Senate report states:
This concern is very easily addressed. The Bill does not ban or prohibit vapes. They will be available to anyone who has a doctor’s prescription and obtainable from a pharmacy. To say that vapes are “banned” or “prohibited” is therefore like saying Australia bans all prescription drugs. If anyone were to say straight-faced that in Australia, antibiotics and the pill are “banned” because they require a prescription, we would know we were dealing with someone with some bizarre agenda. Yet this is the routine way in which extremist vaping advocates speak about current vaping policy.
Whenever I need a repeat prescription for one of the two life-saving drugs I have used for over 20 years, I contact my GP via a prescription renewal app and pick up several months supply at my local pharmacy. On a scale of life’s many inconveniences, I’d rank it way below trying to contact a human at a bank, a telco or utility provider, arranging travel or voting. A very first world problem.
Getting a prescription vape is no different the way we deal with other drugs of dependence. Methadone and buprenorphine are prescribed harm reduction drugs for those with opiate dependence. They are not sold in convenience stores or bong shops. They are most commonly dispensed at pharmacies. It’s the same with the very good analgesic codeine: it’s available on prescription to those who need it. These are not “banned”.
Before February 2018, low-dose codeine was available across-the-counter in Australia in a variety of medications. Following accumulating evidence of abuse, it was then rescheduled to prescription-only access. A wastewater evaluation found codeine use dropped 37% across Australia between 2016 and 2019. Many who were using it who did not need to, stopped using it when access was limited. This was harm reduction in action.
So where were the howls of protest at this heinous blow to the freedom for anyone to use as much codeine as they like?
Vape crusader Alex Wodak is adamant: he’s highly supportive of prescription access to regulated drugs. But he’s apoplectic about vapes being treated the same way.
Concerns were also raised in the Senate enquiry about vapers living in small country towns or isolated rural addresses. How would they access legal prescribed vapes when there was no pharmacy anywhere near where they lived, but there were general stores or petrol stations who could stock vapes?
The answer of course, is that people living in such isolation nearly all use all manner of prescribed drugs too. Doctors do online consultations and pharmacies have long dispensed via mail or courier services. This concern is nothing but rural solidarity posturing which doesn’t survive even cursory interrogation.
Why is there no significant black market in prescribed drugs?
No one in all this seems to have asked a very obvious question. With there being massive demand for a huge range of (not) “banned” prescribed drugs (315 million PBS and RPBS prescriptions in 2020-2021), why has the prescription model of drug access been flourishing for many decades in all but lawless or chaotic nations where you can often pick up almost any drug you want without a prescription?
Why have not Australian “criminal gangs” decided that here was a golden opportunity to supply any of the 925 PBS drugs to people wanting them without the hassle of getting a prescription? Why are we not seeing pharmacies torched by criminal gangs?
There are black markets for some weight loss and male sexual dysfunction drugs and anabolic steroids for men anxious about their muscles. But these are the few exceptions that prove the rule: Australia’s Therapeutic Goods Administration is second to none in world in assuring public access to safe and efficacious drugs, highly subsidised in the case of 925 PBS approved drugs.
Some wet-behind-the-ears contributors have backed a compromise: scheduling vapes as pharmacy-only, but over-the-counter. This would simply hand the same gold pass to vapes that exists now to kids and non-smoking “recreational” vapers. Right now they can front hundreds, perhaps thousands of retail vape shops and online retailers and easily get vapes.
But with no prescription required, any street smart kid will be able to do what kids have long done with cigarettes: with cash ready, ask an older friend or an adult outside a pharmacy to go inside and buy them vapes, Over 18 recreational vapers will just waltz in and buy them.
But critically, this step would also set a dangerous precedent. It would signal that our parliament thinks it’s OK for it to do the job that the TGA’s expertise has been established to do. If they can dictate scheduling for vapes, why stop there? Why not tell the TGA how to schedule any drug that a bunch of politicians with the balance of power thinks should be made more freely available or in other scenarios made unavailable (eg; the morning after pill)
If the Greens vote to tear the prescription access heart out of the Butler bill, they will have carried on the legacy of this bunch of 28 Liberal and National Party backbench political vandals who knee-capped Greg Hunt’s 2022 import ban on vapes, dooming the crippled model to failure by letting cheap, flavoured kid-friendly vapes flood in. They will have helped the Big Tobacco funded Nationals ($340,000 in the last decade from Philip Morris, and $55,000 recently from British American Tobacco), with their ragbag of fellow travellers like Ralph Babet, One Nation and Tammy Tyrell – to have their way.
We’d expect nothing less from that lot, but many of us expect far, far more from the Greens.
If the Greens throw their lot in with this rabble and the Australian Association of Convenience Stores, also partly funded by Big Tobacco, they will have made a statement that retailers which have brazenly broken the law over the past years should now be rewarded by being anointed as official newly-minted, government-approved vape retailers.
“Convenience stores and vape shops: not the problem, the solution!
Those like Wodak advocating for vapes to be sold as “consumer products” by licenced retailers constantly refer to the proliferation of vapes as being supplied by “criminals”. But 2022-23 data on where vapers obtain their vapes, show that 56.5% bought their NVPs from ‘bricks and mortar’ retailers (tobacconists, vape shops, convenience stores, service stations etc). With children, 15.6% buy from shops, with 77.8% obtaining them from family or friends, many of whom bought them from shops too.
This “criminals” language is designed to imply that those knowingly selling illegal NVP products alongside ordinary grocery items are somehow not criminal but respectable, law-abiding, folksy small business people. But the NVPs are supplied to retailers who knowingly sell them illegally by the very bulk importing criminals vaping advocates want us to keep front-of-mind. They act as fences for criminal importers.
Today, the vested interests which loathe and despise the prescription scheme are now in full blown panic mode that they are about to lose their lucrative brazen illegal trade. They have decided their best bet is to inhabit the caring, concerned, faux outraged narrative of how terrible it is that kids can so easily buy vapes from the heinous ‘black market’: vapes that are dangerous to kids because they might come from seedy ‘bathtub and kitchen sink’ chemical workshops in China! Not like the nice clean vapes often made by Big Tobacco that we can provide. Like their cigarettes, these don’t cause health problems. Oh wait …
They have tried to characterise the evil black market as those retailers who have been selling illegal vapes, including to children, whom they contrast with legitimate, law-abiding retailers who would no sooner sell vapes to children that sell their grandmothers for pet food. They are now jostling to stand sanctimoniously in the front line of reform advocacy which would see any retailer who puts their hand up to be a “licensed vape retailer” able to sell.
Holding loud hailers, they chorus “the prescription model has been a huge failure! It’s now time to properly regulate vapes as a legitimate consumer good and let it be sold … well, everywhere by responsible retailers just like us.”
The sheer, galactic gall in all of this is, of course, that many of these “we’re here to help” retailers have been openly breaking the law for years. They now want everyone to have massive amnesia about all this and see convenience stores as not the problem, but the solution. They have openly broken the law at industrial levels but are now wanting governments to believe that there could be no better candidates for responsible, law-abiding vape retailing than them. We would just never sell to children, they chorus.
Support is particularly high in young people, the heartland of Green voting. Cancer Council supported research shows 84% of young Australians support or do not oppose the removal of vapes from retail stores.
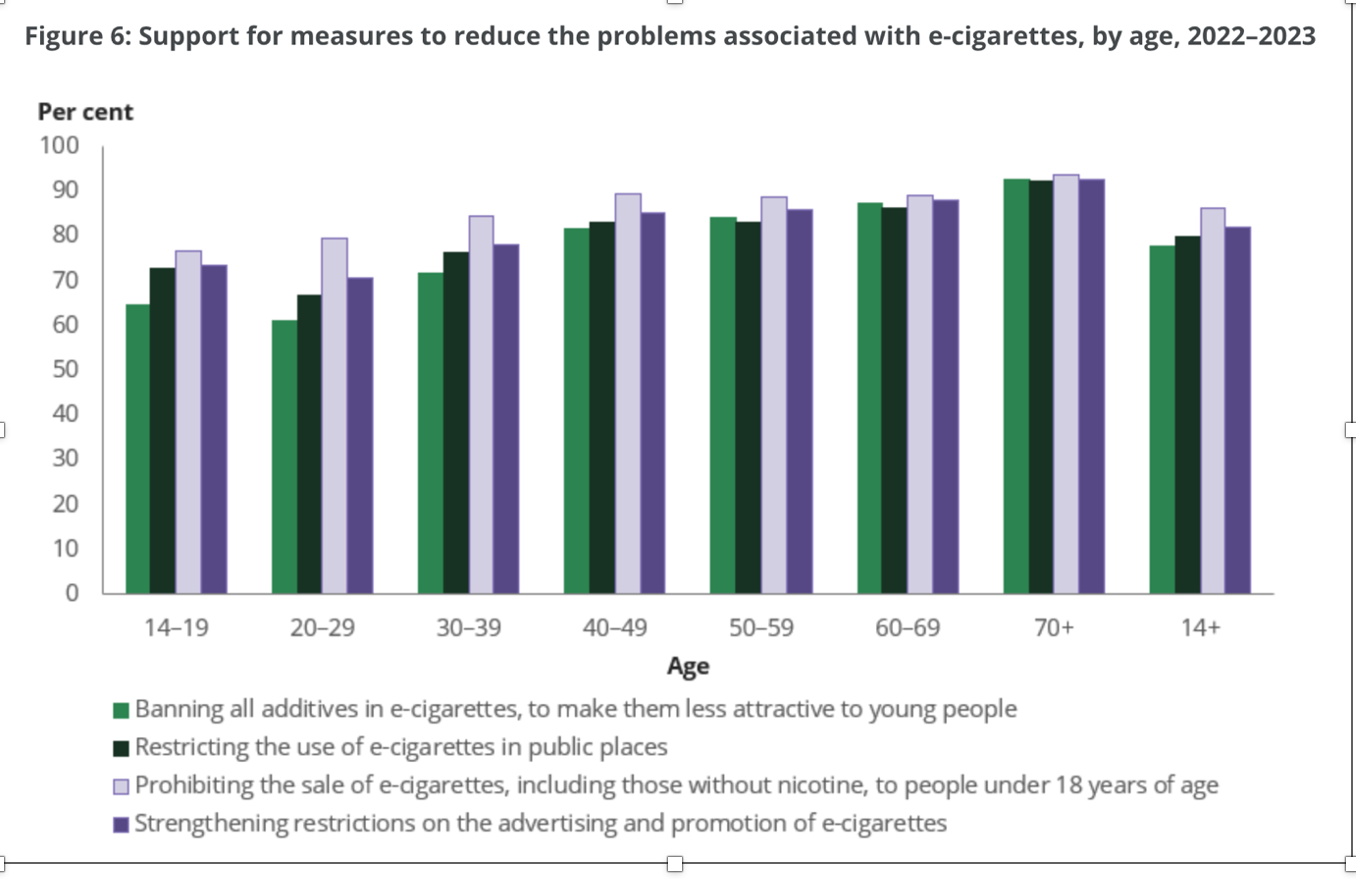
The latest official national data on smoking and vaping in Australia were released in late February. One of the most remarkable sets of findings was the massive support across the community for tough controls on the promotion and supply of vapes (see chart below).
The data were collected between 2022 and May 2023 from some 21,500 people across Australia by the Roy Morgan company, on contract from the Australian Institute of Health and Welfare to conduct the latest in the National Drug Household Survey (NDHS) series, run since 1985.
A question about restricting sales of vapes to those with a prescription was not included. But former health minister in the Morrison government Greg Hunt had announced his support for the TGA recommendation in December 2020. This received widespread news coverage in the three years since, including during the survey period.
Here’s how much the Australian public supports four proposals to reduce youth vaping.
Banning all additives in e‑cigarettes, to make them less attractive to young people: 78%, (question asked for the first time in the 2022–2023 survey)
Restricting the use of e‑cigarettes in public places: 80% – an increase from 69% in 2019.
Prohibiting the sale of e‑cigarettes, including those without nicotine, to people under 18 years of age: 86%, an increase from 79% in 2019.
Strengthening restrictions on the advertising and promotion of e‑cigarettes: 82%, an increase from 67% in 2019.
I’ve tried, but I cannot find any contemporary social issue where there is anything surpassing the overwhelming support for vaping controls shown in the chart above. For example, the 2017 national plebiscite on marriage equality saw 61.7% vote yes. Two thirds of Australians want the government to do more on climate change. In 2022, two in three believed junk food advertising in children’s viewing times should be banned and 70% believe that gambling ads on TV should be banned. But support for tough restrictions on promotion and sale of vaping products is running between 78% and 86%.
But then we have this …
A letter signed by “31 Australian tobacco control and addiction experts” sent to federal politicians on 18 March 2024 stated that “A recent Redbridge Survey found that 84% of adults agree/strongly agree that ‘Nicotine vaping products should only be available through licensed retail outlets to adults’”.
The report of the survey is here. It was commissioned by the Australian Association of Convenience Stores (AACS) whose CEO is a former long-time employee of British American Tobacco. It focuses on industry-supported positions about how vaping products would best be regulated in Australia and shows the data by the 2022 voting choices of those completing the survey. So with this complexion, it was clearly intended by those who commissioned it as an exercise in warning politicians about the possible political repercussions of the government’s legislation being adopted.
So let’s take a walk through it.
First, who is the Redbridge consulting company which is responsible for the survey? Its website states its mission is “helping clients manage political risks through research-led communication and advocacy” and that “We enable clients to influence governments, stakeholders and public opinion to achieve outcomes that provide shared and meaningful benefits.” Redbridge’s pitch to potential clients is nakedly about influencing opinion and policy rather than simply measuring knowledge, attitudes and behaviour in the way that any survey with no agenda would have done.
Redbridge’s mission is to deliver its clients potent data consistent with its clients’ policy objectives that might help foment the clients’ desired outcomes being achieved.
So who then, was the commissioning client for survey? Significantly, the report says nothing about this, a standard inclusion in survey reporting. So we are left to speculate about who forked out for the survey, which would not have been cheap.
Along with the big three tobacco companies in Australia (PMI, BAT and Imperial Brands) which have all declared their opposition to prescription access to vapes) the AACS is a sworn enemy of prescription access. The AACS of course exists to serve the interests of its members in the convenience store channel, most of which sell tobacco. The AACS has a long history of tobacco industry support, with tobacco companies paying premium top-tier membership fees. All tobacco companies are heavily invested in vapes.
Convenience stores have been one source of supply of vapes in Australia with approximately 8.5% of consumers reporting that they’d purchased nicotine vaping products from convenience stores despite it being illegal to sell vaping products containing nicotine outside the prescription arrangements. They desperately want that river of gold to keep flowing into their shops. Effective enforcement of Australia’s longstanding laws on prescription medicines will end their ability to sell vapes openly, and the large penalties for selling proposed amendments currently under consideration by the Parliament are likely to deter the great majority of retailers from doing so.
The report does not show the actual questionnaire
While the Redbridge report takes us through responses to questions asked in the survey, it provides no copy of the exact questionnaire used, showing the order of the questions. In surveys, ordering can be critical in framing and conditioning respondents’ understanding of and responses to subsequent questions. Critically here, the industry-supported position that vapes ‘should be regulated like alcohol and tobacco’ was asked without any alternative policies being presented or contextualised. Without such alternatives, many respondents who are likely to have no detailed understanding of the alternatives and their rationale, would have their response options powerfully framed by this comparison with alcohol and tobacco regulation.
The prescription regulatory model used for restricting access to addictive drugs like codeine, methadone and pseudoephedrine (and indeed to all prescribed drugs) is the clear and obvious alternative here. There are very few cases of retailers selling of prescription drugs by those not authorised to do so (registered pharmacists).
If as seems likely, this question appeared early in the questionnaire, this placement would make it highly likely that many would agree with that proposition in the absence of any alternative options. As we saw in the NDHS survey, almost all Australians want more effective action to stop illegal vape sales. So having agreed that the regulatory models used for alcohol and tobacco were the way to go at the beginning of the survey, many respondents would want their subsequent responses to be consistent with what they had responded earlier, biasing their consideration through to the end of the survey.
Who were the sample of people who completed the questionnaire?
The report simply states that the respondents were “recruited over online panel” using quotas forage, gender, location, education and vote at the 2022 federal election. So we know nothing from the report about how the online panel came to be assembled. How were they recruited? What were the refusal rates to join the panel and to engage with this survey on vaping? How was the survey’s scope and purpose described to them? Were they told who had commissioned the survey? If not, why not? Were they paid? The absence of this basic information is concerning.
Question asked: Do you agree or disagree with the following statement? Regulated nicotine vaping products should only be available for sale to persons aged 18 and above through licensed retail outlets, the same as alcohol and tobacco products.
The tobacco and convenience store lobbies want prescription access scrapped and instead the licensing of vape retailers. It is doubtful that many respondents would be aware that tobacco retailers are already licensed/registered in six Australian jurisdictions or that it has always been illegal to sell nicotine vapes to anyone and to sell non-nicotine vapes to those under 18 years. Such sales are enormous despite this illegality.
Between 2019 and 2023, the proportion of young people buying e-cigarettes directly from tobacco retailers went up—from 7.1% to 16.8% of 14–19 year-old users and from 12.5% to 26.1% in 15–24 year old users The proportion of 18-24 years old users who reported purchasing from a tobacco retail outlet increased from 13.7% to 30.1% (Table 3.39). Among those 18-24, fewer than 10% of young reported using vapes sold as not containing nicotine (Table 3.18), so the vast majority of sales to young people in all these groups would have been illegal either because they were under 18 and/or because the vapes contained nicotine. [Tables here].
An informative preamble to the question should have been worded like this:
“Tobacco retailers are licensed or registered in six Australian states and territories. It is already illegal to sell nicotine vapes to anyone without a prescription, yet the latest data show that tobacco retailers are major sources of purchasing vapes despite this illegality. Given this, doyou agree or disagree with the following statement? Regulated nicotine vaping products should only be available for sale to persons aged 18 and above through licensed retail outlets, the same as alcohol and tobacco products.”
This would have provided respondents with highly relevant information critical to answering the question.
How many respondents may have supported the general sales model and how many the pharmaceutical supply model as their preferred option had they been presented with the following data?
Use of highly biased information in preamble
In the preamble to the question about the preferred model,a statistic is used that would clearly bias respondents against the plan that the Government should tighten laws to ensure that the prescription-access model actually works. It states that despite restrictions, the “National Illicit Drug Reporting System survey has found only 3% of vapers have a nicotine prescription, with 97% of nicotine vapers purchasing illegally.”
Few if any respondents would have any knowledge about what the NIDRS study is. It is not a population representative survey. It is a study tracking behaviour among a group of regular illicit drug users, not the whole population. So it is a group of people quite different to the population as a whole. Use of prescriptions is much higher among the general public, as shown in a 2022 survey of adults in Victoria, and the 2022-23 NDHS.
This information would suggest that nearly all vapers are choosing to not buy their vapes via prescription. This would hardly be surprising, given that none of the Government’s new enforcement measures came into place until 2024, whereas the Redbridge survey was conducted in February 2024. Vapes remain readily available today, with no penalty to either users or retailers (the latter being simply due to lack of enforcement).
But in any case, it is hardly surprising that high numbers of people reported purchasing from tobacco and other retailers selling illegally. None of the Government’s new enforcement measures relating to local sale or supply will come into force until later in 2024, whereas this survey was conducted in February 2024. Vapes remain readily available today, with no penalty to either users or retailers (the latter being simply due to current lack of feasible enforcement).
In summary, the Redbridge survey ticks many boxes as a deliberate effort to secure data that serve the commissioning sponsors’ commercial agenda of discrediting the prescription access model and showing that Australians think regulating access to vapes should learn nothing from the catastrophic errors across 120 years of allowing tobacco to be sold literally everywhere.
This has been achieved by biased and incomplete preambles to questions that do not allow respondents relevant information and which would likely deflate their glib assumption that teenage vaping is a problem that can be sold by handing the official keys to “regulated” vaping to the very retail sectors which have knowing and brazenly broken the law for years.
How many of the 31 signatories actually read the survey?
The list of 31 “expert” addiction and tobacco control signatories to the letter to politicians contains many names who have no or next to no track record in population-focussed tobacco control. Across my 40+ years in tobacco control I have never seen most of them in any meeting, conference, forum or committee concerned with any aspect of tobacco control. And across 17 years of editing the BMJ’s Tobacco Control , I saw very few of them ever submit a single paper to the journal.
Their views on vaping control are as relevant as mine would be on a political letter about (say) the best way to reform pill testing at music festivals.
The dominant group among the signatories are those with illicit drug professional backgrounds who appear to have little understanding of the detail of tobacco control policy, its history and achievements, and the short and long game strategies of those highly motivated to jeopardise those achievements.
But their signatures on the political letter also suggest many of them did not even look at the survey their names blessed by their gesture. They should be embarrassed.
The NHHS data above suggest that any major political party failing to acknowledge this unprecedented support will alienate a large proportion of the community if it seeks to respond to the vaping epidemic with self-serving options being cheered on by the vaping, tobacco and convenience store industries.
Other blogs in this series
Vaping theology: 1 The Cancer Council Australia takes huge donations from cigarette retailers. WordPress 30 Jul, 2020
Vaping theology: 2 Tobacco control advocates help Big Tobacco. WordPress 12 Aug, 2020
Vaping theology: 3 Australia’s prescribed vaping model “privileges” Big Tobacco WordPress Feb 15, 2020
Vaping theology: 4 Many in tobacco control do not support open access to vapes because they are just protecting their jobs. WordPress 27 Feb 2021
Vaping theology: 5 I take money from China and Bloomberg to conduct bogus studies. WordPress 6 Mar, 2021
Vaping theology: 6 There’s nicotine in potatoes and tomatoes so should we restrict or ban them too? WordPress 9 Mar, 2021
Vaping theology: 7 Vaping prohibitionists have been punished, hurt, suffered and damaged by Big Tobacco WordPress 2 Jun, 2021
Vaping theology: 9 “Won’t somebody please think of the children”. WordPress 6 Sep, 2021
Vaping theology: 10: Almost all young people who vape regularly are already smokers before they tried vaping. WordPress 10 Sep, 2021
Vaping theology: 11 The sky is about to fall in as nicotine vaping starts to require a prescription in Australia. WordPress 28 Sep, 2021
Vaping theology: 12 Nicotine is not very addictive WordPress 3 Jan 2022
Vaping theology 13: Kids who try vaping and then start smoking,would have started smoking regardless. WordPress 20 Jan, 2023
Vaping theology 14: Policies that strictly regulate vaping will drive huge numbers of vapers back to smoking, causing many deaths. WordPress 13 Feb, 2023
Vaping theology 15: The government’s prescription vape access scheme has failed, so let’s regulate and reward illegal sellers for what they’ve been doing. WordPress 27 Mar 2023
Vaping theology 16: “Humans are not rats, so everybody calm down about nicotine being harmful to teenage brains”. WordPress 13 Jul, 2023
Vaping theology 17: “Vaping advocates need to be civil, polite and respectful” … oh wait. WordPress 3 Oct, 2023
Vaping theology 18: Vaping is a fatally disruptive “Kodak moment” for smoking. WordPress Oct 30, 2023
Vaping theology 19: Vaping explosions are rare and those who mention them are hypocrites. WordPress 17 Nov, 2023
Vaping theology 20 : Today’s smokers are hard core nicotine dependent who’ve tried everything and failed – so they need vapes. WordPress 14 Dec, 2023
Vaping theology 21: Australia’s prescription vapes policy failed and saw rises in underage vaping and smoking. WordPress 10 Jan, 2024
Vaping theology 22: “Prohibition has never worked at any point for any other illicit substance”. WordPress 17 Mar 2024
Vaping theology 23: “84% of the Australian public are opposed to the way the government will regulate vapes” WordPress 2 Apr, 2024
The Australian government with support from all the states and nearly every health and medical agency in the country, has introduced a policy that requires all vapers to have a prescription for these products which can only be dispensed by a registered pharmacist. In 2021/22, 223.1 million prescriptions subsidised by the Pharmaceutical Benefits Scheme (PBS) were filled in a population of some 26 million.
There can be few who do not get a prescription dispensed at least each once a year. In our two-person house, we take seven drugs between us. It’s a routine part of nearly all our lives. Oral contraceptives, statins, blood pressure and diabetes control drugs, strong pain relief and asthma control drugs are among those most commonly used.
If anyone were to tell you that in Australia, antibiotics and the pill are “banned” because they require a prescription, you would look past them knowing you were dealing with someone with some bizarre agenda. Yet this is the routine way in which extremist vaping advocates and their few remaining megaphones in the media speak about current vaping policy.
Nicotine is an addictive drug, and it has always been illegal for vape shops and tobacconists to sell nicotine vaping products in Australia. It’s a law that has been widely ignored by retailers who have pretended that they only sell vapes without nicotine. On repeat, proponents of e-cigarettes drone on that the Government has banned vapes and that this is “prohibition”. However, what happened in 2021 was a loosening of supply, not a ban. Far from ‘prohibition’ the changes were intended to ensure that people who wanted to use vapes to try to quit could legally do so, so long as they had a prescription. Unfortunately, retailers exploited that loosening of restrictions and sales of nicotine vaping products have exploded. To make the law work, the Government has recently stopped people importing vapes, just as entrepreneurs cannot import (eg) for example, Viagra or flog strong pain medications in convenience stores. But they will still be available to anyone who wants to use them for help with quitting or nicotine addiction.
Changes are common to the scheduling of drugs. For example, before February 2018, low-dose codeine, a very useful opiate for pain relief, was available across-the-counter in Australia in a variety of medications. Following accumulating evidence of abuse, it was then rescheduled to prescription-only access. A wastewater evaluation found codeine use dropped 37% across Australia between 2016 and 2019. Many who were using it who did not need to, stopped using it.
Despite the roll-out of the new policy being far from complete, a piece in The Australian this week was headlined Australia’s vape ban has utterly failed. What now? The article forgot to mention the rather elephantine-sized obvious point that vaping retailers have until July 1, 2024 to sell off any remaining stock they have. That’s why we still see vapes on sale in many shops today. This next phase of the plan is to ensure kids no longer walk past vapes shops on their way to school, no longer have fruity pink vapes sold to them in the very same shops selling lollies, fizzy drinks and ice cream. Without this crucial next piece of legislation being passed, retailers will simply continue to flout the law and our prescription model will never get the chance to be implemented as intended.
The same thing happened when plain packs were introduced in 2012: there was a grace period when old stock could be sold off before this finally became illegal. Vape advertising has long been banned and imports on vapes not destined for the pharmacy trade were banned from March 1. After July 1, retailers will risk massively deterrent fines, with prosecutions by the states and the TGA.
It is the situation that has operated for the past three years that has been impossible to enforce. The new reforms being introduced will actually make enforcement possible. Retailers transacting vape sales through shops, market stalls, or on-line need to let customers know how to contact them to get vapes. These routes will now fully expose those sellers who can no longer hide behind the cover of non-nicotine vapes. If a teenage kid can work out how to get vapes, those experienced in investigating illegal sales of any sort will find it child’s play. Many retailers will see it as simply too risky.
The Australian article also failed to mention why the policy failed so badly under the Morrison government when its prototype was first introduced by former LNP health minister Greg Hunt. A back bench revolt lead by Matt Canavan and Hollie Hughes, aided by luminaries like Barnaby Joyce, Eric Abetz, Tim Wilson and James Paterson, gutted the Hunt policy by leaving the prescription access pillar intact, but overturning the import bans. This was like entering a three-legged horse in the Melbourne Cup. But all this is never mentioned by those dancing around the corpse of the Hunt reforms.
Mark Butler’s policy has reinstated the twin pillars of the Hunt policy and extended them to include non-nicotine vaping products (because these falsely-labelled items were being used as a legal defence by retailers (“the pack said no nicotine, m’lud. How was I as an honest shopkeeper trying put a roof over my family’s head, supposed to know this was incorrect?”) It “bans” vapes in the same way that the government “bans” all prescription drugs.
“Everyone knows” prohibition doesn’t work
It is a commonplace for people, including some wet-behind-the-ears ‘experts’, to solemnly declare that prohibition never works. But such claims rarely specify what the test of failure actually means. Is random breath testing, introduced in Australia in 1976, a failure because every day people are still charged with being over the limit? Or is zero drink driving the only meaningful test of its importance? All governments across the last 48 years seem to agree that zero cases would be a preposterous standard against which to assess impact, knowing that there have been huge reductions in alcohol-caused driving fatalities in that time. Illicit drugs of course are still procurable in all countries in which they are illegal. Tiny percentages of Australian school students reported using opiates and methamphetamine in the last month of the most recent national survey (see table). But 14.5% (nearly 1 in 7) 14-17 year olds have vaped in the past month
I asked my 14-year old granddaughter if she knew where her friends buy vapes. She did. I know she would be clueless about how to buy heroin, cocaine or meth. By contrast, for the last few years vapes have been sold cheaply and openly in every suburb and country town. So if a small number of clandestine sellers find ways to keep selling vapes after July 1, will this mean the policy has “utterly failed”, as the Australian screamed?
Alcohol and drugs research maven Emeritus Professor Wayne Hall from the University of Queensland commenced his 2010 review in Addiction of the lessons to be learned from alcohol prohibition in the USA with “ ‘Everyone knows’ that national alcohol prohibition in the United States between 1920 and 1933 was a quixotic and failed social experiment”.
In his erudite myth-busting review, Hall examined this factoid (unreliable information that is reported and repeated so often that it becomes accepted as fact) and its implications for policy debates about “bans” on alcohol. He concluded “It is incorrect to claim that the US experience of National Prohibition indicates that prohibition as a means of regulating alcohol is always doomed to failure. Subsequent experience shows that partial prohibitions can produce substantial public health benefits at an acceptable social cost, in the absence of substantial enforcement.”
His review and this piece suggest that prohibition was associated with a number of positive social and economic changes while it lasted, and that the almost universally accepted “fact” that it caused widespread growth in the black market for alcohol and in associated crime and corruption may in fact have been phenomena only documented for a small number of cities.
Beverage alcohol can be quite easily made, as the popularity of home brewing and wine-making attests. But the manufacturing of vaping equipment is something very few people would be capable of doing, particularly in commercial quantities. Shutting down retail access outside of pharmacies is highly unlikely to see burgeoning hobbyist manufacturing networks set up. Where would they acquire the oceans of liquid nicotine, for a start?
Dr Alex Wodak, an unswerving advocate for open access to vaping products, argued recently that “Vaping is to smoking what methadone is to street heroin.” Correct. But curiously Wodak failed to note in his comment that methadone is only available via special prescription authority, dispensed at some pharmacies and clinics.
In 2021, 70.6% of Australia’s 47,500 methadone patients received their methadone at a pharmacist. Some keep obtaining it illegally, but there are no sensible calls for this system to be axed, let alone for methadone to be sold in corner shops.
In fact Wodak says he has never advocated that methadone should be available to whoever wants to buy it from any retailer wanting to sell it, in just the way that cigarettes can be sold and in the way he believes vapes should also be sold. He believes that drugs like opiates and “all prescribed drugs” which are acutely toxic and capable of causing serious health consequences quickly including death, should appropriately be restricted to medical oversight.
But addiction to nicotine causes the death of over 8 million people a year because without nicotine in tobacco, very few would ever smoke.
In Australia and elsewhere governments ban many things: child pornography, semi-automatic firearms, mace and pepper sprays, flick knives, dynamite, DDT, asbestos, often accompanied by the wailing of aggrieved libertarian consumers who want to “choose” to have these things. Consumer protection legislation has banned and regulated 1000s of both acute and chronically dangerous goods, chemicals and set standards for emissions etc. Many of these exposures do not cause disease quickly, but over long periods of time. Wodak’s rationalisation that only agents capable of causing rapid toxic effects should be medically regulated is blind to the massive dominance of chronic disease in modern health problems.
If cigarettes were invented tomorrow, no government would allow them to be sold with the knowledge we have today of their health effects. So what should this teach us about vaping? That we should learn nothing from the disaster of allowing tobacco to be sold as freely as it is?
A 2021 statement by 15 past presidents of the Society for Research into Nicotine and Tobacco declared “High-quality clinical and epidemiological data on vaping’s health effects are relatively sparse. There are no data on long-term health effects, reflecting the relative novelty of vaping and the rapid evolution of vaping products. Determining even short-term health effects in adults is difficult because most adult vapers are former or current smokers.”
We do not know the net health effects of vaping and will not know them for decades, just as occurred with the slow emergence of knowledge of the health effects of smoking and breathing in asbestos particles.
Mark Butler’s policy on vaping will again stamp Australian governments as being in the front row of the grid of nations which have dared to stand up to Big Tobacco. Every major tobacco company in the world has invested heavily in vapes while leaving its feet firmly on the throttle of promoting smoking as well. All are implacably opposed to Mark Butler’s policy. That’s all we need to know.
Other blogs in this series
Vaping theology: 1 The Cancer Council Australia takes huge donations from cigarette retailers. WordPress 30 Jul, 2020
Vaping theology: 2 Tobacco control advocates help Big Tobacco. WordPress 12 Aug, 2020
Vaping theology: 3 Australia’s prescribed vaping model “privileges” Big Tobacco WordPress Feb 15, 2020
Vaping theology: 4 Many in tobacco control do not support open access to vapes because they are just protecting their jobs. WordPress 27 Feb 2021
Vaping theology: 5 I take money from China and Bloomberg to conduct bogus studies. WordPress 6 Mar, 2021
Vaping theology: 6 There’s nicotine in potatoes and tomatoes so should we restrict or ban them too? WordPress 9 Mar, 2021
Vaping theology: 7 Vaping prohibitionists have been punished, hurt, suffered and damaged by Big Tobacco WordPress 2 Jun, 2021
Vaping theology: 9 “Won’t somebody please think of the children”. WordPress 6 Sep, 2021
Vaping theology: 10: Almost all young people who vape regularly are already smokers before they tried vaping. WordPress 10 Sep, 2021
Vaping theology: 11 The sky is about to fall in as nicotine vaping starts to require a prescription in Australia. WordPress 28 Sep, 2021
Vaping theology: 12 Nicotine is not very addictive WordPress 3 Jan 2022
Vaping theology 13: Kids who try vaping and then start smoking,would have started smoking regardless. WordPress 20 Jan, 2023
Vaping theology 14: Policies that strictly regulate vaping will drive huge numbers of vapers back to smoking, causing many deaths. WordPress 13 Feb, 2023
Vaping theology 15: The government’s prescription vape access scheme has failed, so let’s regulate and reward illegal sellers for what they’ve been doing. WordPress 27 Mar 2023
Vaping theology 16: “Humans are not rats, so everybody calm down about nicotine being harmful to teenage brains”. WordPress 13 Jul, 2023
Vaping theology 17: “Vaping advocates need to be civil, polite and respectful” … oh wait. WordPress 3 Oct, 2023
Vaping theology 18: Vaping is a fatally disruptive “Kodak moment” for smoking. WordPress Oct 30, 2023
Vaping theology 19: Vaping explosions are rare and those who mention them are hypocrites. WordPress 17 Nov, 2023
Vaping theology 20 : Today’s smokers are hard core nicotine dependent who’ve tried everything and failed – so they need vapes. WordPress 14 Dec, 2023
Vaping theology 21: Australia’s prescription vapes policy failed and saw rises in underage vaping and smoking. WordPress 10 Jan, 2024
Vaping theology 22: “Prohibition has never worked at any point for any other illicit substance”. WordPress 17 Mar 2024
Vaping theology 23: “84% of the Australian public are opposed to the way the government will regulate vapes” WordPress 2 Apr, 2024
This is a lengthy two part podcast on vaping hype, published on 6 Feb 2024 on Karl’s Shirtloads of Science podcast. In it, I discuss the factoid that vaping is “95% safer than smoking”; critically look at claims that vaping is the most effective way of quitting smoking; at what vapers inhale deep into their lungs when they vape; and discuss Australia’s historic policy of requiring vapes to be sold only to those with a doctor’s prescription.
I’ve done 1000s of interviews over my 45 year career. This I think is one of the best.
I have a dear friend who has lived with strong pain every day and night for over a decade. Following extensive damage to her spine from osteoporosis, she was advised to have a spinal fusion operation, on threat of needing a wheelchair for the rest of her life. She has a metal “cage” supporting her lower spine but pain fills her life. More often than not, she wakes several times a night and gets some relief from hot showers. Pain relieving drugs are a daily part of her life. Globally, millions of people live with unremitting pain. If you are in pain, it dominates your life.
I originally published this piece (below) in the Sydney Morning Herald, 18 September, 1999. It was republished in a collection of 71 of my writings on health Smoke Signals, in 2016.
In 1809, 47 year old Jane Crawford risked scalping and the tomahawk to ride her horse 60 miles in four days to the practice of Dr Ephraim McDowell in Danville, Kentucky. Mrs Crawford’s ovarian tumour was giving her unremitting, labour like pain. While several men held her arms and legs, and she recited psalms, McDowell took 25 minutes to cut a 14cm incision in her lower belly, remove a 1.2kg tumour and then sew her up with interrupted sutures. Outside the house, an angry and incredulous mob not unlike those who would today seek to close heroin injecting rooms that minister to a different sort of pain, waited ready to lynch McDowell should his patient die. Five days later she was out of bed and lived for another thirty years.
McDowell’s pioneering operation and his patient’s courage are historical landmarks in the annals of surgery.
While opium and cocaine have been used since antiquity for pain relief, it was not until 1846 when Thomas Morton first used ether to anaesthetise a patient for a tooth extraction that lengthy and detailed surgery more subtle than crude hacking could be performed under general anaesthesia. The next year, chloroform was used for the first time to relieve pain in childbirth and went on to become the anaesthetic of choice for more than a century. Today, pain management specialists estimate that more than 90% of postsurgical, post-trauma and cancer pain can be fully relieved, and 75% in chronic, non-cancer pain such as arthritis. Thirty years ago, these figures hovered around 10%. Worldwide though, only half those suffering from these conditions have access to services and drugs which can provide this relief.
Proust wrote that “Illness is the doctor to whom we pay most heed: to kindness, to knowledge we make promises only; pain we obey.” People in pain are preoccupied by the experience. Pain bulldozes all emotions aside, including hope. Yet pain produces a bewildering range of ambivalence. While aspirin and paracetamol are the most commonly used drugs, and around one in five experience pain that has lasted longer than three months, so often we conspire to deny the reality of pain. We feel obliged to cheer the injured footballer who returns to the fray after losing teeth or being knocked unconscious. Many couples make a virtue out of refusing pain relief in childbirth. While a woman begs for an epidural, her husband gently counsels “remember we agreed … no drugs”. Many who have lived with pain tell of the scepticism of others (“You don’t look like you’re in pain”) but also of the subtle imperatives to stop their misery infecting those around them. Anglo and Asian women tend to be stoic in childbirth, while southern European and Arabic women are uninhibited in their expression. Moralists, including many in medicine, have often denied the dying sufficient morphine, fretting that they might become addicted.
Recently, television allowed us to consider the abandoned Serbian torture chamber, where unspeakable degradations were wrought on its Kosovar captives. Torture is the active infliction of pain on its unwilling victims. Professor Michael Cousins, head of the Pain Management Research Centre at Sydney’s Royal North Shore Hospital, describes unrelieved pain as “torture by omission”. The United Nations Declaration of Human Rights codifies civilised society’s most basic standards and aspirations for its citizens.
Yet as Cousins points out, the Declaration says nothing about the most elemental concern of all: the right to be relieved from pain.
This remarkable omission is a testimony to our ambivalence about pain. Its consequence is that pain management as a medical speciality lives a Cinderella existence, shining occasionally as islands of enlightenment in a sea of misery. The most recent and exciting developments involve discoveries about the way that damaged nerve endings sprout pain fibres, the growth of which can be inhibited and so the pain controlled through drugs administered through surgically implanted mini pumps. People who have lived for years in desperate pain are now being assisted to live largely pain-free lives again through such developments. Yet there are only seven pain management training centres in Australia, and for all the pious political talk of the need for palliative care after the overturning of the Northern Territory euthanasia legislation, cruelly token budgets have found their way into health expenditure in the period since.
As historically unprecedented falls in fecundity, better living standards and the successes of public health combine to cause the age distribution of the world’s populations to balloon increasingly to the right of the graph, more people will live with the pain of chronic degenerative conditions and cancer. Despite this, the disabling and all-absorbing nature of pain often militates against its victims becoming potent advocates for pain relief to be declared a basic human right, and all that would flow from this. If Cousins’ and his colleagues’ mission were to succeed, what a gift to the world this would be.
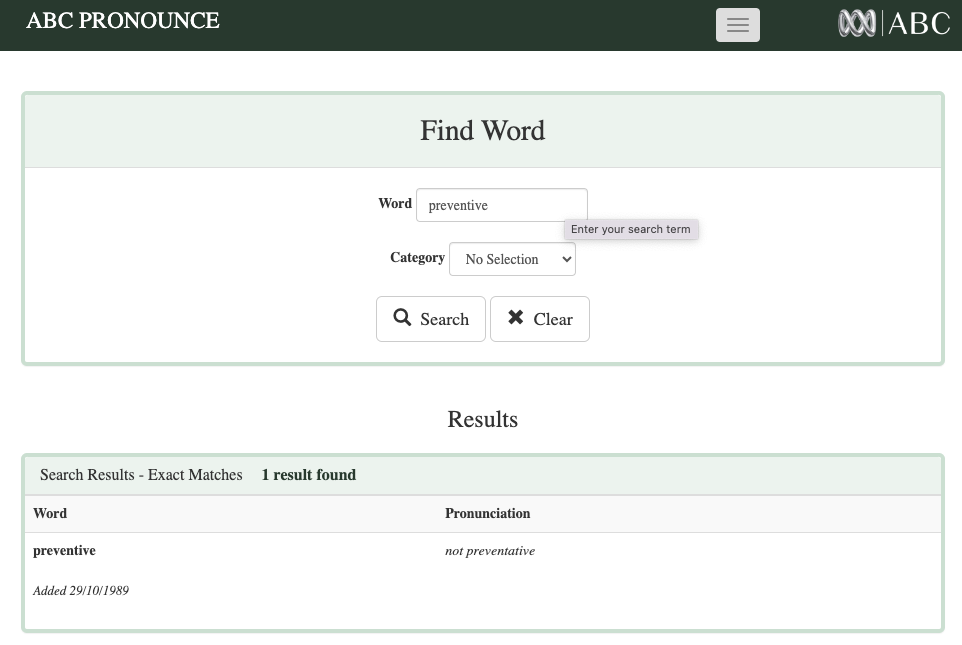
I write to draw attention to the pernicious creep of “preventative” instead of “preventive” in what the ABC broadcasts. Your pronunciation standards guide, ABC Pronounce, formally notes that “preventive”, not preventative be used. This ruling has been in place since 1989.
Tonight on the Sydney 7pm news bulletin, the words “preventative medicine” bannered an item on vaping. I’ve noticed it several times recently.
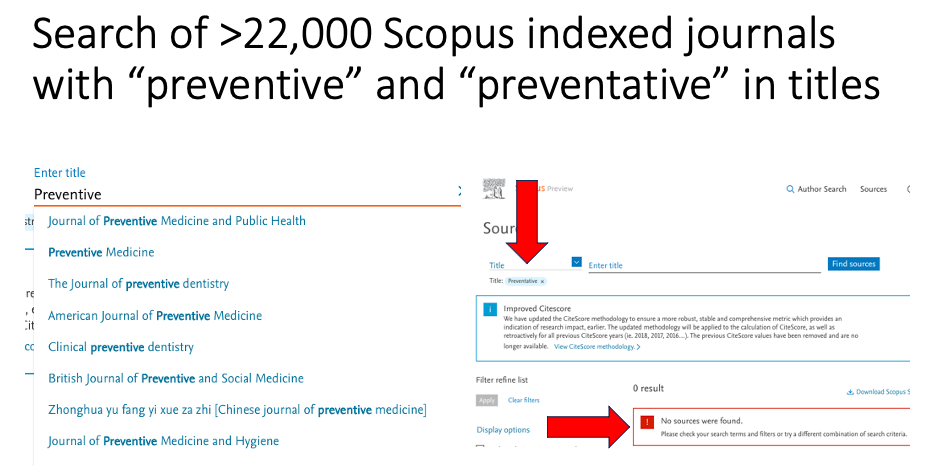
Scopus, the scientific world’s largest and most respected scholarly reference service indexes over 22,000 journals. Not one of these has the word “preventative” in its title, but there are 10 with “preventive” (see https://www.scopus.com/sources.uri)
The School of Public Health at the University of Sydney was the first school of public health in Australia and the first to offer a Masters in Public Health (in 1978). At the time it had a Department of Preventive and Social Medicine. I was on the staff from the first intake of students and today have an emeritus appointment in the School.
Across 45 years, there have been countless times when staff in the School have rolled their eyes and corrected students’ essays and treatises by changing “preventative” to “preventive”. “Preventative” is an infectious Americanism which has attained its currency by brute force of repetition. It grates in the ears of anyone working in this field . I’d put it in the same league as the American pronunciation of “defence” (“dee-fence”). I’ve never heard an American official refer to the US Department of Dee-Fence, yet the dee-word is endemic in sports commentators.
Sorry, but anyone who pairs “preventative” with “medicine” immediately marks themselves as someone who has never actually worked in preventive medicine.
The knock-out argument here is this: there is no verb to “preventate”. We simply prevent things and in public health, preventive medicine is a major division in the discipline of public health.
When the definitive history of tobacco control is written, it will record a most peculiar phenomenon. British tobacco control experts cannot help themselves from schooling Australian colonial numbskulls about where we are going so very wrong with vaping. Britain really has better vaping policy than Australia, they keep telling us.
This is quite amusing because as we’ll see below, some 10 years after the major boom in vaping commenced, vaping prevalence is higher in Britain than in Australia and you could put a cigarette paper between the smoking prevalences of the two countries. And in the last 30 years, Australia has always had the gall to implement nearly every major policy change ahead of Britain. So that’s quite a herd of elephants in the room.
Pro-vaping English researchers and advocates have often written submissions to government enquiries in Australia where they tried to explain England’s superior track record. It’s all a bit like the equivalent of Britain’s fanatical one-eyed Barmy Army cricket supporters who insist that England – not Australia – really won the 2023 Ashes series; that England’s Jonny Bairstow should not have been given out stumped in the 2023 second test at Lords; that England really were the best team at the 2023 One Day World Cup, despite coming seventh below even the Afghanistan minnows while Australia humiliated an apparently invincible India in the final.
This has been going on for some time, Australia and England have met in 361 test matches since 1877. Australia has won 152 and England 112, with 97 ending in draws.
So what about smoking and vaping? With tobacco control, there is almost nothing in recent decades that the Poms had the initiative or mettle to introduce before Australia showed them the way. They have always been the bridesmaids. Here are a few examples:
Graphic health warnings: Australia followed the 2000 lead of Canada in introducing graphic picture health warnings on packs in 2006. Britain implemented them in Oct 2008.
Pub smoking bans: Australian states and territories began banning smoking in pubs from 1998, Britain did it in July 2007
Plain packaging: Australia implemented it Dec 1 2012, the world’s first. Britain: in May 2017.
Smokeless tobacco ban: Australia June 1991; Britain in 1992 (following a EU Tobacco Products Directive)
Price of cigarettes: Australia #1 in the world ($US25.88 a pack); UK #2 ($US15.83 – 39% less)
Retail display bans:NSW got the ball rolling in July 2008, with all states subsequently following. England and Wales: from 26 May 2015.
English apoplexy over Australia’s prescription access to vapes
“[F]irst, rigorous enforcement of the ban on vapes and snus sales to children and young people under 18, with punitive measures for non-compliance; second, ban the sale of snus and vapes to adults except when prescribed for smoking cessation, as, in our experience, wider availability enables them to fall into children’s hands; and third, introduce a total ban on disposable vapes.”
All three measures are central to Australia’s recently announced policy on vaping.
So how did England’s leading tobacco control advocacy group react to this call? Deborah Arnott, chief executive of health charity Action on Smoking and Health (ASH) was quoted in a press report on the paediatricans’ letter as saying: “ASH wants action to curb youth vaping, but making vapes only available on prescription won’t help, after they tried this in Australia underage smoking and vaping both went up … Australia’s aggressive anti-vaping policy opened the door to illegal vapes, conflated the harms of vaping with smoking and left tobacco cigarettes, which are far more harmful, on sale everywhere. ASH supports evidence-based measures to curb youth vaping, by prohibiting branding and marketing appealing to children. The disposable vapes that have surged in popularity in recent years are available for pocket money prices on every street corner and they’re currently packaged more like a sweet or a toy than a smoking cessation device. This is unacceptable and must change.”
So let’s take a look at Arnott’s ignorance of what has actually happened in Australia, and her formidable abilities to walk on both sides of the street at once.
She says Australia “tried this” (ie prescription access to vapes) and then “underage smoking and vaping both went up”.
Predictably, this saw the surviving prescription access component fail to be taken up by nearly all Australian doctors and vapers. Why would smokers bother to go to a doctor to get a script for vapes when they – plus legions of non-smokers including kids who were “recreationally vaping” — could buy vapes easily right across the country?
This failure had nothing to do with the prescription access component, but everything to do with the useful idiots in the far right of politics and their urgers in vaping advocacy who held the national door open for unrestrained illicit trade.
Notably too, all this happened during the COVID pandemic, when state and federal governments seconded thousands of health department hands to be on deck for COVID-related duties. As a result, the requirement that vapes could only be sold to those with a prescription was almost totally ignored by retailers, knowing that its policing was being accorded all but zero priority by health departments. You could buy vapes almost anywhere. Just like you have always been able to do in Britain. Imagine what would have happened if pharmacies decided to ignore the law and sold prescribed drugs to anyone wanting them. Pharmacists would have been struck off, or even jailed.
Arnott appears to have dined out on the huge propaganda campaign designed to discredit the politically gutted prescription policy internationally, straight from the industry’s playbook it tried (and badly failed) to use in stopping the spread of plain packaging legislation
And then she says that Australia shockingly “left cigarettes on sale everywhere” while it attempted to implement prescription access. Ermmm … just like Britain and every other nation in the world has left them on sale everywhere! This is the same old populist knee-jerk reaction we have seen about every significant piece of tobacco control policy “this is window-dressing! If you’re really serious about stopping smoking, why don’t you just ban cigarettes”.
I dealt with the wittering myopia of this argument in an earlier blog. The argument that you cannot seriously regulate vapes (as Australia is now doing) for as long as cigarettes are sold to anyone over 18 would have to be among the most cringeworthy, forelock tugging pieces of defeatism in contemporary public health.
I have often heard public health leaders say “If cigarettes were invented today, and we knew all we know about their dangers that we know now, not a country in the world would allow them to be sold.” Well, Trump’s America might. It took more than half a century of smoking for us to understand the full risks of smoking. Those who run this argument are effectively saying “let’s learn nothing from the history of smoking-caused disease and its control, let’s just let vaping rip like we did with cigarettes and cross our fingers about any down-the-track consequences”.
Restricting access to vapes through prescription allows smokers with serious intent to quit smoking another option. Importantly, a homeopathically small number of doctors would issue children or non-smokers with scripts for vapes, whereas they can access them with ease under Arnott’s preferred policy.
Opponents of prescription access – especially those interests centred on selling vapes to as many people as possible – have megaphoned the alleged “failure” of Australia’s prescription policy. It speaks volumes about the arrogance of English tobacco control, that the head of its oldest advocacy agency is apparently so clueless about what actually happened in Australia.
ASH England supports “adults only” targeted vaping marketing
She continues: “ASH supports evidence-based measures to curb youth vaping, by prohibiting branding and marketing appealing to children.”
This is truly gob-smacking stuff. When I started in tobacco control in the late 1970s, the main challenge was getting rid of tobacco advertising and promotions. The tobacco industry ran the argument on repeat for over a decade that there was such a thing as tobacco advertising that appealed to adults but not to children. We should let that bloom, they argued, but jump on not ads that beguiled kids. Some never-specified, surely magic barrier prevented “adult” advertising messages from ever penetrating the orbits of children. No one in the advertising industry had ever heard of such barriers.
UK legislation on permitted vaping advertising is classic, absurd “half pregnant” policy: ads are banned on radio, television and magazines, but not in cinemas, posters, leaflets or bus sides. The UK Government has been advised that British kids apparently never go to the movies, see billboards or see buses when they pass.
In 2024 Deborah Arnott has climbed in her tardis, inviting us to believe in the same tooth fairy “evidence-based” controls when it comes to neutering vape marketing to kids.
And then we need to ask why, if vaping is as benign to health as its advocates claim it is, do they nonetheless feel bound to say that they want to “curb youth vaping”. Why not treat vaping like yo-yos, hula hoops, fidget spinners and other harmless childhood fads, as a leading pro-vaping Australian advocate once suggested. Seriously.
In Australia in 2022, one in ten (10.6%) adults were current daily smokers. This rate has steadily declined from 22.4% in 2001. This report did not provide data on less than daily current smoking prevalence. However an earlier (different) national survey showed that another 1-2% smoke not daily but less than monthly. So the two countries are about the same.
Vaping In Britain 8.7% of adults currently vape daily or occasionally, an increase from 2021 where 7.7% of people reported daily or occasional e-cigarette use. Vaping is highest among those aged 16 to 24 years in Great Britain; the percentage of people in this age group who were daily or occasional vapers in 2022 has increased to 15.5%, up from 11.1% in 2021.
In Britain in 2023, 20.5% of children 11-17 had tried vaping, up from 15% in 2022 with 7.6% currently vaping, up from 6.9%.
In Australia, there has been a far more dramatic increase between 2017 and 2022/23 in both “ever” vaping and current (past month) vaping in school children aged 12-17. Just under 30% of Australian school students have now tried vaping. The figure below shows a significant fall in exclusive smoking that is in line with the historic trend downward. In 2017 9.7% of students were either exclusively vaping or vaping and smoking (dual using) while in 2022-23 this had shot up to an alarming 16%, more than 1 in 6.
Given that only 7.3% of students were exclusively smoking and/or dual using in 2017, it follows that the lion’s share of the increase in vaping has occurred in children who had never smoked: they had taken up vaping not as a substitute for smoking, with some undoubtedly also then also taking up smoking (longitudinal studies show that children who take up vaping have a three-fold greater probability of later taking up smoking).
As we saw above, Britain has played catch-up with Australia on almost every tobacco control policy. Like Australia, it has seen rapid growth in vaping by children, many of whom have never smoked. And like Australia, it has seen historic falls in smoking by children which long preceded the advent of vapes. Our adult smoking rates are about the same, while Australia’s adult vaping prevalence is half that of Britain’s.
This all raises serious questions about which population groups are being most affected by vaping. Vaping prevalence is rising far more than smoking prevalence is falling. So claims that vaping is a population-wide game changer in smoking cessation are clearly hype. But there is unequivocal evidence that the present arrangements for vaping access are seeing massive rises in kids being exposed to the addictive highly drug nicotine. This is no accident but as central to the vaping industry’s business plan as securing smoking in successive cohorts of teenagers was to the tobacco industry (where today, every company is heavily invested in vapes).
These data underscore the importance of the Australian government’s policies to get vapes out of the reach of kids by making them prescription access only.
Other blogs in this series
Vaping theology: 1 The Cancer Council Australia takes huge donations from cigarette retailers. WordPress 30 Jul, 2020
Vaping theology: 2 Tobacco control advocates help Big Tobacco. WordPress 12 Aug, 2020
Vaping theology: 3 Australia’s prescribed vaping model “privileges” Big Tobacco WordPress Feb 15, 2020
Vaping theology: 4 Many in tobacco control do not support open access to vapes because they are just protecting their jobs. WordPress 27 Feb 2021
Vaping theology: 5 I take money from China and Bloomberg to conduct bogus studies. WordPress 6 Mar, 2021
Vaping theology: 6 There’s nicotine in potatoes and tomatoes so should we restrict or ban them too? WordPress 9 Mar, 2021
Vaping theology: 7 Vaping prohibitionists have been punished, hurt, suffered and damaged by Big Tobacco WordPress 2 Jun, 2021
Vaping theology: 9 “Won’t somebody please think of the children”. WordPress 6 Sep, 2021
Vaping theology: 10: Almost all young people who vape regularly are already smokers before they tried vaping. WordPress 10 Sep, 2021
Vaping theology: 11 The sky is about to fall in as nicotine vaping starts to require a prescription in Australia. WordPress 28 Sep, 2021
Vaping theology: 12 Nicotine is not very addictive WordPress 3 Jan 2022
Vaping theology 13: Kids who try vaping and then start smoking,would have started smoking regardless. WordPress 20 Jan, 2023
Vaping theology 14: Policies that strictly regulate vaping will drive huge numbers of vapers back to smoking, causing many deaths. WordPress 13 Feb, 2023
Vaping theology 15: The government’s prescription vape access scheme has failed, so let’s regulate and reward illegal sellers for what they’ve been doing. WordPress 27 Mar 2023
Vaping theology 16: “Humans are not rats, so everybody calm down about nicotine being harmful to teenage brains”. WordPress 13 Jul, 2023
Vaping theology 17: “Vaping advocates need to be civil, polite and respectful” … oh wait. WordPress 3 Oct, 2023
Vaping theology 18: Vaping is a fatally disruptive “Kodak moment” for smoking. WordPress Oct 30, 2023
Vaping theology 19: Vaping explosions are rare and those who mention them are hypocrites. WordPress 17 Nov, 2023
Vaping theology 20 : Today’s smokers are hard core nicotine dependent who’ve tried everything and failed – so they need vapes. WordPress 14 Dec, 2023
Vaping theology 21: Australia’s prescription vapes policy failed and saw rises in underage vaping and smoking. WordPress 10 Jan, 2024
Smokers have been trying to quit since smoking started, and there have always been opportunists trying to cash in on those hopes. A 1923 book published in Melbourne, Secret Recipes,described an “anti-smoking mixture” where 36 grains of silver nitrate were mixed with 475ml of water for use as an aversive mouthwash after meals. A medical advice column in the Detroit News from 1949 also recommended the same path, “One trying to quit smoking should exclude from his diet meat soups, broths or extracts, highly seasoned sauces or dishes. He or she should eat freely of apples, baked with meals or raw the first thing for breakfast and the last thing at night.”
Such folksy hokum persisted for decades in leaflets and tip sheets often provided by health departments. For example, this Ugandan advice from 2004 counselled: “Nature has the remedy. Stretch out your arm and pick up a carrot. Chew it and smile. Within a few hours, all your distress will be gone. This orange root has large amounts of charm that is appropriate for those who wish to give up smoking.”
Enter NRT
The advent of prescription-only nicotine replacement therapy (NRT) from the late 1980s and its more than 30 years of subsequent widespread use, marked the first time that large-scale efforts promoted medication to assist quitting. Prior to NRT, those who ‘took something’ to help them quit used preparations that made money for the patent medicine spruikers selling them, but none of the snake oils touted by their commercial and moral evangelists ever saw them in widespread use.
However, very large numbers of smokers began quitting when news reports of the first serious case-control studies started being published from the early 1950s. In 1955, just five years wide news publicity was given to Wynder and Graham’s historic study in JAMA of smokers and lung cancer in the same year as the BMJ Doll and Hill paper on smoking and lung cancer, 7.7 million Americans aged 13 and over (6.4% of the population) were former smokers. Ten years later in 1965, following further widespread publicity surrounding the 1964 US Surgeon General’s Report, the number of ex-smokers had ballooned to 19.2 million (13.5% of the population aged 13 and over were ex-smokers). At the Second World Conference on Smoking and Health held in London in 1971, Daniel Horn, the director of the US National Clearinghouse on Smoking and Health, presented results of a cohort of 2,000 US smokers interviewed in 1966 and again in 1970. Twenty six per cent of men and 17% of women had stopped smoking for a year or more across this time. Horn noted that 99% had done so without any formal help: “The level of change in smoking habits in the United States has become quite massive and I regard it as a change in health behaviour that is largely dependent on individual decision.”
By 1975, 32.6 million Americans (19.4%) had stopped smoking. Quitting smoking had become a major phenomenon. In 1979, the then director of the US Office on Smoking and Health noted in a National Institute of Drug Abuse Monograph “In the past 15 years, 30 million smokers have quit the habit, almost all of them on their own.” Many of these quitters had been very heavy smokers.
The only tobacco control policy in place for around a decade from the mid 1960s in a tiny handful of vanguard nations were tepid, general and very small health warnings on cigarette packs and low-key and poorly funded education via posters and pamphlets. The main drivers of all the quitting described above had been news publicity about the dangers of smoking. This gave millions a why to quit. They figured out the how for themselves and nearly all of it was unassisted.
Reportage of the 1986 US national Adult Use of Tobacco Survey was set against the dramatic fall in smoking prevalence from 40% in 1965 to 29% in 1987. Yet again, the central finding was that smokers who quit overwhelmingly did so unaided:
“About 90% of successful quitters and 80% of unsuccessful quitters used individual methods of smoking cessation rather than organized programs. Most of these smokers who quit on their own used a ‘cold turkey’ approach.”
“Double your chances of quitting”
I worked in tobacco control in the years when NRT first appeared in the 1980s. The big pitch repeated endlessly in pharmaceutical company publicity for decades was that smokers could “double their chances” of quitting if they used NRT, then the only potentially mass-reach method of quitting. But what this beguiling soundbite concealed was that this “doubling” was the relative increase compared with placebo or those in trials who used no aids. The absolute increase was utterly dismal: at 6 to 12 months follow-up, those using NRT and other pharmaceutical aids typically did only marginally better than those smokers not using them, with the bottom line being that there were few drugs in the whole of medicine which had such an abject “success” rate.
As I wrote in an earlier blog summarising a Cochrane meta-analysis of vaping vs NRT randomised controlled trials “if we take 100 smokers participating in an RCT, 90 would still be smoking six months later if they used e-cigarettes, compared with 94 who used NRT, and 96 who just tried to quit alone or got some “behavioural support”… If you went along to your doctor for a health problem and were told ‘here, take this. It has a 90% failure rate. But I’m describing it as successful.’ …what would you think?”
My (free, open-access) 2022 book Quit Smoking Weapons of Mass Distraction explores at length the history and determinants of the cessation dogma that smokers are foolish to try to quit unaided, despite the paradox that this is exactly how two-thirds to three quarters of all long term ex-smokers have finally succeeded in stopping.
Enter the “hardened” smoker
In the first decade of this century, debate began about whether, after four decades of widespread publicity on the dire risks of smoking, and burgeoning tobacco control policies designed to reduce smoking, those who still smoked should now be best described “hardened”. The “hardening hypothesis” proposed that as the prevalence of smoking in a population declines, those still smoking will be hardened: average number of cigarettes smoked daily will be rising, fewer smokers will be making successful quit attempts and measures of nicotine dependence will be heading north.
Since that time many studies have tested this hypothesis. Two recent reviews of these have concluded that the hypothesis is now well and truly dead and buried.
A 2020 review by smoking cessation maven John Hughes of published studies on hardening found that in none of the 26 studies he examined was there any evidence for a reduction in conversion (or transition) from current to former smoking, in the number of quit attempts, or success on a given quit attempt, with several studies finding that these measures increased over time. These results appeared to be similar across survey dates, duration of time examined, number of data points, data source, outcome definitions and nationality. Hughes concluded “These results convincingly indicate hardening is not occurring in the general population of smokers” in nations where smoking prevalence is falling.
A 2022 systematic review of three reviews and ten repeat cross-sectional studies found all but one concluded a lack of hardening. Most found softening within the smoking population, consistent across hardening indicators, definitions, countries (and tobacco control environments), and time periods examined.
The authors concluded: “Based on the weight of the available evidence, the “hardening hypothesis” should be rejected and the reality of softening accepted.” So as smoking falls in a population, we see the exact opposite of hardening: the remaining smokers smoke less than in eras when smoking was more prevalent, make more successful quit attempts.
Enter vaping
Those promoting vaping have been ignorant of or undeterred by the death of the hardening hypothesis. They have dug up its grave, put lipstick on the corpse and announced ad infinitum that today’s smokers simply “can’t” quit smoking either on their own or with any other available method. Their evidence is always anecdotal in the form of passionate testimonies from those who read from the hardening script.
It is undoubtedly true that there are some – even quite a lot – of highly nicotine dependent smokers whose failed quitting history and wish to quit is difficult to dispute. In Australia, these smokers are able to access nicotine vapes via prescription, with the same ease that 315 million prescriptions for all drugs were dispensed in a population of 25 million.
But importantly, when we look at the young adult age groups which vapes the most, we find a huge number of Australians who currently vape (i.e. in the last month) who have never smoked. Then there are dual users (smokers who also vape), many of whom dual use for many years showing no sign of this being a transitory phase in an eventual switch to vaping. I’ll be covering this in a forthcoming blog. Health minister Mark Butler calls these “recreational users”: vapers who either have never smoked or who vape and continue smoking across several years, showing no obvious resolve to quit (they are “won’t quits”, not “can’t quits”).
What’s obvious here is that while a much greater proportion of young smokers vape than do non-smokers, because there are so many more non-smokers, even their lower vaping rates translate into there being more numbers of non-smokers who currently vape than smokers who currently vape (53% v 47%).
More recent data (2022) for those aged 18+ are also available for Victoria. In that study, a quarter of all current e-cigarette users were never smokers (25.0%), 28.7% were former smokers, and almost half (46.3%) were also current smokers (ie dual users).
The proportion of never smokers who currently use e-cigarettes increased 4.5- fold from 0.6% in 2018-19 to 2.7% in 2022. This represents approximately 77,200 never smokers who reported currently vaping, of which 44,534 (more than half – 57.7%) were under the age of 25 years. These data would bring great delight to vaping manufacturers, particularly those tobacco transnationals which sell both cigarettes and vapes. Here was a product that not only had little impact on helping smokers quit in the population, but one that caused many smokers to now purchase both cigarettes and vapes. As if this was not huge enough, it also – without precedent – was demonstrably drawing more non-smokers into nicotine addiction, than it was keeping smokers in theirs.
Other blogs in this series
Vaping theology: 1 The Cancer Council Australia takes huge donations from cigarette retailers. WordPress 30 Jul, 2020
Vaping theology: 2 Tobacco control advocates help Big Tobacco. WordPress 12 Aug, 2020
Vaping theology: 3 Australia’s prescribed vaping model “privileges” Big Tobacco WordPress Feb 15, 2020
Vaping theology: 4 Many in tobacco control do not support open access to vapes because they are just protecting their jobs. WordPress 27 Feb 2021
Vaping theology: 5 I take money from China and Bloomberg to conduct bogus studies. WordPress 6 Mar, 2021
Vaping theology: 6 There’s nicotine in potatoes and tomatoes so should we restrict or ban them too? WordPress 9 Mar, 2021
Vaping theology: 7 Vaping prohibitionists have been punished, hurt, suffered and damaged by Big Tobacco WordPress 2 Jun, 2021
Vaping theology: 9 “Won’t somebody please think of the children”. WordPress 6 Sep, 2021
Vaping theology: 10: Almost all young people who vape regularly are already smokers before they tried vaping. WordPress 10 Sep, 2021
Vaping theology: 11 The sky is about to fall in as nicotine vaping starts to require a prescription in Australia. WordPress 28 Sep, 2021
Vaping theology: 12 Nicotine is not very addictive WordPress 3 Jan 2022
Vaping theology 13: Kids who try vaping and then start smoking,would have started smoking regardless. WordPress 20 Jan, 2023
Vaping theology 14: Policies that strictly regulate vaping will drive huge numbers of vapers back to smoking, causing many deaths. WordPress 13 Feb, 2023
Vaping theology 15: The government’s prescription vape access scheme has failed, so let’s regulate and reward illegal sellers for what they’ve been doing. WordPress 27 Mar 2023
Vaping theology 16: “Humans are not rats, so everybody calm down about nicotine being harmful to teenage brains”. WordPress 13 Jul, 2023
Vaping theology 17: “Vaping advocates need to be civil, polite and respectful” … oh wait. WordPress 3 Oct, 2023
Vaping theology 18: Vaping is a fatally disruptive “Kodak moment” for smoking. WordPress Oct 30, 2023
Vaping theology 19: Vaping explosions are rare and those who mention them are hypocrites. WordPress 17 Nov, 2023
This was also a week where Mendelsohn, with “the greatest humility” let us know that he was gonged with a coveted award from the UK Vaping Industry Association (UKVIA) as their new public health golden boy.
In his blog, he helpfully explained UKVIA’s impact on smoking:
Col also updated his website FAQs (see under ‘fires and explosions’) with a generally sensible series of tips on how to prevent your vape exploding. But he just couldn’t resist adding a photo of me and my electric vehicle.
His tag-team partner in sophistry, someone who goes on and on and on about the need for civility, politeness and respect, helped out by making the relevance of the photo explicit in a subsequent tweet.
Exploding vapes have grabbed headlines for good reason, as this show-reel of incidents illustrates. Here’s a 2018 review of 164 cases on e-cigarette explosion injuries. 35% resulted in second degree burns and 20% in third degree burns (the worst), with many necessitating skin grafts. The most common sites were thighs, hands, face and genitals.
But when it comes to catastrophic risk, it’s explosions on aircraft that are most concerning. The US Federal Aviation Administration (FAA) advises that any device using lithium batteries should be stored in carry-on luggage. But its regulations only prohibit a small range of devices from stowed luggage and these include … you guessed it … electronic cigarettes and vapes. Now why would that be? Because as they explain:
“Electronic smoking devices, like vapes and e-cigarettes, contain lithium batteries and are considered dangerous goods due to their risk of smoke, fire and extreme heat. As such, they are restricted to on how they can be packed when preparing for travel on an aircraft. These devices were the leading cause of lithium battery incidents on aircraft in 2022.”
The potential consequence of an intense heat vape battery fire deep in the hold of a crowded airliner is dire.
But hey, what would the world’s largest airline regulator know, when Col and Alex think it’s all just “exploiting fear” to mention explosions as a concern?
Yes, I drive an electric vehicle. And undoubtedly just like both Mendelsohn’s and Wodak’s, my house is also full of appliances that use lithium batteries: laptops, tablets, mobile phones, power banks, torches, remote controls, fitness monitors, and power tools. When these products very rarely catch on fire, we typically see highly publicised global recalls like this laptop, these power tool batteries and the infamous Samsung Galaxy Note 7.
But Google couldn’t show me any examples of recalls for exploding vapes. This almost certainly reflects the cowboy nature of vast segments of the vaping manufacturing industry and the thousands of equally dodgy retailers willing to stock them.
Electric vehicles have much lower probability of catching fire than internal combustion engine (ICE) vehicles. From 2010-2023 EV FireSafe has verified 393 EV battery fires globally. To put this in context, there are some 30 million EVs on the world’s roads. This Conversation review points to fires in ICE vehicles being some 80 times more common than in EVs. Tesla’s 2020 impact report argued that there was one Tesla fire for every 330 million kilometres their vehicles have travelled. Tesla automatically collects full kilometer and incident data for every car it has ever sold, across all owners.
After reading about the explosion risks of vapes and EVs, I’m very pleased to warm my nether regions in winter driving on the Tesla’s battery powered seat warmers rather than risk molten lithium trickling around my testicles if I vaped. Goodness, gracious great balls of fire!
Wodak’s apparent understanding of the comparative risks and consequences of vape explosions with those occurring in EVs seems about as informed as his unforgettable comparison of nicotine in tobacco with that in vegetables like eggplants and potatoes, the most opened of all blogs in this series.
Hypocrisy? Not guilty m’lud.
Other blogs in this series
Vaping theology: 1 The Cancer Council Australia takes huge donations from cigarette retailers. WordPress 30 Jul, 2020
Vaping theology: 2 Tobacco control advocates help Big Tobacco. WordPress 12 Aug, 2020
Vaping theology: 3 Australia’s prescribed vaping model “privileges” Big Tobacco WordPress Feb 15, 2020
Vaping theology: 4 Many in tobacco control do not support open access to vapes because they are just protecting their jobs. WordPress 27 Feb 2021
Vaping theology: 5 I take money from China and Bloomberg to conduct bogus studies. WordPress 6 Mar, 2021
Vaping theology: 6 There’s nicotine in potatoes and tomatoes so should we restrict or ban them too? WordPress 9 Mar, 2021
Vaping theology: 7 Vaping prohibitionists have been punished, hurt, suffered and damaged by Big Tobacco WordPress 2 Jun, 2021
Vaping theology: 9 “Won’t somebody please think of the children”. WordPress 6 Sep, 2021
Vaping theology: 10: Almost all young people who vape regularly are already smokers before they tried vaping. WordPress 10 Sep, 2021
Vaping theology: 11 The sky is about to fall in as nicotine vaping starts to require a prescription in Australia. WordPress 28 Sep, 2021
Vaping theology: 12 Nicotine is not very addictive WordPress 3 Jan 2022
Vaping theology 13: Kids who try vaping and then start smoking,would have started smoking regardless. WordPress 20 Jan, 2023
Vaping theology 14: Policies that strictly regulate vaping will drive huge numbers of vapers back to smoking, causing many deaths. WordPress 13 Feb, 2023
Vaping theology 15: The government’s prescription vape access scheme has failed, so let’s regulate and reward illegal sellers for what they’ve been doing. WordPress 27 Mar 2023
Vaping theology 16: “Humans are not rats, so everybody calm down about nicotine being harmful to teenage brains”. WordPress 13 Jul, 2023
Vaping theology 17: “Vaping advocates need to be civil, polite and respectful” … oh wait. WordPress 3 Oct, 2023
Vaping theology 18: Vaping is a fatally disruptive “Kodak moment” for smoking. WordPress Oct 30, 2023