

Dr Colin Mendelsohn recently published a co-authored paywalled paper in Addiction comparing smoking and vaping prevalence in adults and adolescents in New Zealand and Australia during 2016-2023, when smoking fell in both nations and vaping rose under two different nicotine vaping products regulatory regimes.
Mendelsohn has summarised the paper here and in an opinion piece in the Sun Herald where he modesty declared the paper to be a “landmark” study. The principal policy question driving the paper is whether countries with more restricted access policies on vapes such as Australia with its pharmacy-only access see different changes in smoking than those with more permissive “regulated market models” (RMMs) such as their comparator case study, New Zealand.
Notably, all but one of the Mendelsohn group authors have histories of often strident public advocacy for vapes to be sold to adults through a wide range of registered retailers. These could include dedicated vape stores and tobacconists and any type of retail business. They have relentlessly opposed Australia’s policy of pharmacy-only access to vapes, including in submissions to governments. This has aligned them with advocacy and submissions from all the major tobacco transnationals, right wing think tanks, the convenience store and tobacco retailing industries, Pauline Hanson’s One Nation and the National parties. It has also set them apart from all major medical and public health agencies, every state and the commonwealth health department and a large majority of Australian researchers and public health advocates who strongly supported the government’s proposals (see table).

Their paper concludes that New Zealand’s greater reductions in adult smoking may suggest a causal relationship between higher rates of vaping with higher falls in smoking, concluding “adopting the New Zealand model for vaping is likely to assist Australia in reaching its [smoking reduction] target earlier.” Below I critique three issues which I believe make this conclusion less robust than it may seem. The concerns are:
- Cherry-picking one comparator nation when other RMM nations of equally obvious relevance present far less persuasive evidence
- A pollyannish, naïve or ill-informed view of the ability of RMMs to reduce illegal trade in vapes
- Use of dated smoking prevalence data in modelling forecasts to declare Australia is likely to miss its 2030 target of less than 5% smoking prevalence
I argue below that Australia’s pharmacy access model preserves access to vapes for adult smokers trying to quit in a retail environment where sales to children are highly unlikely because of professional pharmacist ethics. Illegal sales are widespread in nations with RMMs, while ex-pharmacy sales of prescribed drugs are marginal. Pharmacies have long histories of managing access to narcotics and other drugs with misuse or abuse potential such as methadone and codeine.
- Why compare only two nations?
Fundamentally, the stunningly obvious question demanding to be asked is why the authors selected only two nations from which to base their conclusion that a regulated consumer access model is superior to what they call “highly restrictive” models like Australia’s. There are many nations which allow vapes to be freely sold to adults. Three other nations which also largely share the comparable demographic and multi-cultural backgrounds and history of strong tobacco control of Australia and New Zealand justified by the authors for selecting New Zealand and Australia are the UK, the USA and Canada.
Comparing smoking rates between nations is fraught with problems summarised here. These especially include differences in definitions of “smoking” (some defining only cigarettes, others counting any combustible product) and in different reported age ranges (14+, 15+, 18+). Nations like the UK and the USA which count only cigarette use underestimate true exposure to combusted tobacco smoke (smoking), particularly where use of tobacco in water pipes and cigarillos is widespread.
With smoking prevalence being very low in adolescents in each of these nations, those which include under 18s in their total smoking prevalence data like New Zealand, Canada, and the UK will thereby dilute their total point prevalence figures compared to nations which only count 18 and over smokers of all combustibles. Patterns may also differ depending on whether it is daily, weekly or any current smoking that is being tracked, and whether current smoking includes smoking less frequently than monthly.
Point prevalence of current smoking from the latest available data sets for the five nations are:
Australia (10.5%, 14+, all combustibles, 2022-23 National Drug Strategy Household Survey)
Australia (11.1%, 18+, all combustibles, 2022-23 National Drug Strategy Household Survey)
Canada (10.9%, 15+, all cigarettes only, 2022 Canadian Tobacco and Nicotine Survey)
New Zealand (8.4%, 15+, all combustibles, 2023/24 New Zealand Health Survey)
UK (10.5%, 16+, cigarettes only. 2023 Opinions and Lifestyle Survey,)
UK (11.9%, 18+, cigarettes only 2023 Annual Population Survey)
USA (11.6%, 18+, cigarettes only, 2023 National Health Interview Survey)
Additionally, in Europe where vapes are often openly sold, average data from all EU member states for 2019 show daily smoking prevalence of 18.4% in those aged 15+.
The margins of error around these numbers, together with them each being obtained from different starting ages and defining smoking differently, make direct comparisons problematic.
With declining smoking being the primary focus of Mendelsohn et al’s paper, why were these other three nations each with permissive retail RRMs not also compared for the lessons they might equally hold for Australia? With highly liberal vape retail access occurring as much, if not more, in the UK, USA and Canada as in New Zealand, and smoking prevalence in all five nations declining, any putative causal generalisation about the downward effect on smoking of liberal versus restricted retail access becomes immediately contentious. By selecting only New Zealand for comparison with Australia, the authors have cherry-picked a nation to provide a comparison compatible with their previous outspoken advocacy for RRMs.
Similar regulations on retailing vapes in other RMMs
Vaping advocates often describe New Zealand as having the most preferred regulatory model for vapes. Retailers like supermarkets, ‘dairies’ and petrol stations are allowed to sell vapes, but only in limited flavors like tobacco, menthol, and mint. Licensed ‘specialist’ vape retailers can sell a wider range of flavours. However, in practice New Zealand is little different to the UK, the USA and Canada. All have age restrictions on selling, and unlike Australia, all allow retailers engaged in any type of retailing to sell vapes after simply registering.
UK: There are no restrictions on types of retailers which can sell vapes to those aged 18+ in premises or on-line. All products must comply with the Tobacco and Related Products Regulations by only selling products that are notified and compliant with the Medicines and Healthcare products Regulatory Agency specifications.
USA: Vapes assessed by the FDA as suitable for sale can be sold by any retailer to those aged 21+. Twenty-one of 50 states require a permit or retail license to sell vapes.
Canada: Vapes can be sold by anyone with a vaping product licence. Those eligible need only meet financial transparency and probity criteria.
Australia: While Australian consumers were able until 2021 to import nicotine vaping liquid with a prescription, it has never been legal to sell nicotine vapes in Australia. However this was rarely if ever enforced, with vapes being often displayed and openly sold in shops. COVID caused health departments to reallocate staff to COVID-related duties, severely curtailing surveillance and inspection of illegal NVP selling. The fact that non-nicotine vapes were legal to sell until July 2024 made enforcement difficult both at the border and at retail. From mid-2023 a trickle of enforcement commenced, but illegal retailing remains widespread. The Government’s 2024 package of reforms to reinforce a pharmacy dispensing model for supply of vaping products in Australia is wide-ranging. It includes
- Restricting the supply of vaping products to pharmacists, with a prescription required for higher dose products (>20mg/ml <100mg/ml), for people under 18 (and for all customers in Western Australia and Tasmania)
- Requirement for discussion with a health professional about other quitting options, to counsel against dual use and to encourage cessation of vaping
- Banning disposable, flavoured vapes that have proved attractive to children
- Requiring pharmaceutical style packaging to reduce appeal to and risk of accidental poisoning for children
- Limiting chemical additives to a small range of approved flavours
- Standards for electrical safety
- A pre-registration system to allow authorities to investigate suspected instances of failure to comply with standards
- Enforcing legislation prohibiting sale of vapes from other sorts of retail outlets, including on-line sales
Some of this package will not be fully implemented until July 2025. So what is being compared to New Zealand in the Mendelsohn paper is not the full Australian model, but rather the very unsatisfactory situation in Australia which preceded it—the situation which allowed widespread sales which is what the very recently introduced reform package is intended to address.
As with pharmaceuticals, alcohol, firearms and explosives, surveillance and enforcement is necessary under every regulatory model. With so many more products needing to be scrutinised and retailers to be monitored, enforcement under a RRM presents far more challenges than a pharmacy-only model.
Pharmacists have long been granted exclusive rights to dispense prescribed and scheduled drugs. While ex-pharmacy supplies of restricted drugs and supply to those without a prescription are occasionally prosecuted, any non-pharmacist retailer who flagrantly decided to supply prescription drugs to the public would be rapidly investigated, prosecuted and likely suffer severe penalties. This is very much not the experience with the illegal supply of vapes in all the four RMM nations named.
- Do regulated market models reduce illegal sales of vapes?
A purported major benefit of regulated consumer markets for vapes is said to be that they will reduce illegal trade. Mendelsohn et al state “there is no evidence of a significant organised illicit market for vapes in New Zealand” citing a submission to the Australian parliament by two of their group authors which asserted “There is little incentive to operate an illicit supply chain at any commercially viable scale due to effective competition from the legal marketplace.”
This pollyannaish, naïve or ill-informed statement sits awkwardly with recent New Zealand government prosecutions for illegal sales and a controlled purchasing exercise where 10% of 600 tobacco retailers were selling to children. Copious international evidence exists of rampant illicit trade in the UK, USA (market research firm Circana estimates that in 2024 sales of unauthorised, flavoured disposable vapes in the US amounted to 35% of the $6.8 billion worth of e-cigarettes sold in tracked convenience stores and supermarkets. And this estimate does not include massive on-line sales or those from vape shops. The FDA puts the proportion of vapes being sold in the US which do not have a required FDA marketing order at 86.4% — see graph below) and Canada where illegal sales outnumber legal sales in one province amount 36-45% in three others. Canada has an RMM. These dramatic data repudiate claims that RMMs prevent illegal supply.

The Canadian convenience store industry recently stated low-cost tobacco products have become a “major selling feature” for well-known and established organized criminal groups such as the Hell’s Angels. “It is absolutely organized crime at the highest level. It’s a billion-dollar industry for (organized criminal groups). It involves all the levels of violence, and extortion and gangsterism that comes along with it.”
This is in a nation where cigarettes that are taxed less than in Australia vapes can be legally sold by anyone with a permit (see graph below).
- Will Australia likely miss its 2030 smoking reduction target?
The Mendelsohn paper concludes by saying:
“Australia’s current trajectory and a daily rate of 8.3% indicate it is likely to miss its target of 5% daily smoking or less by 2030”. Here they cite two modelling papers which drew on reports published prior to the availability of the most recently data used by the authors in their paper. Australia’s 2022/23 National Drug Strategy Household Survey reported daily adult prevalence at 8.3%, down from 11% in 2019 (an absolute fall of 2.7% and relative fall of 24.5%). This was the largest decline in smoking prevalence reported in 10 triennial NDSHS surveys since they commenced in 1998. As such, it may represent a step change in the decline in smoking.
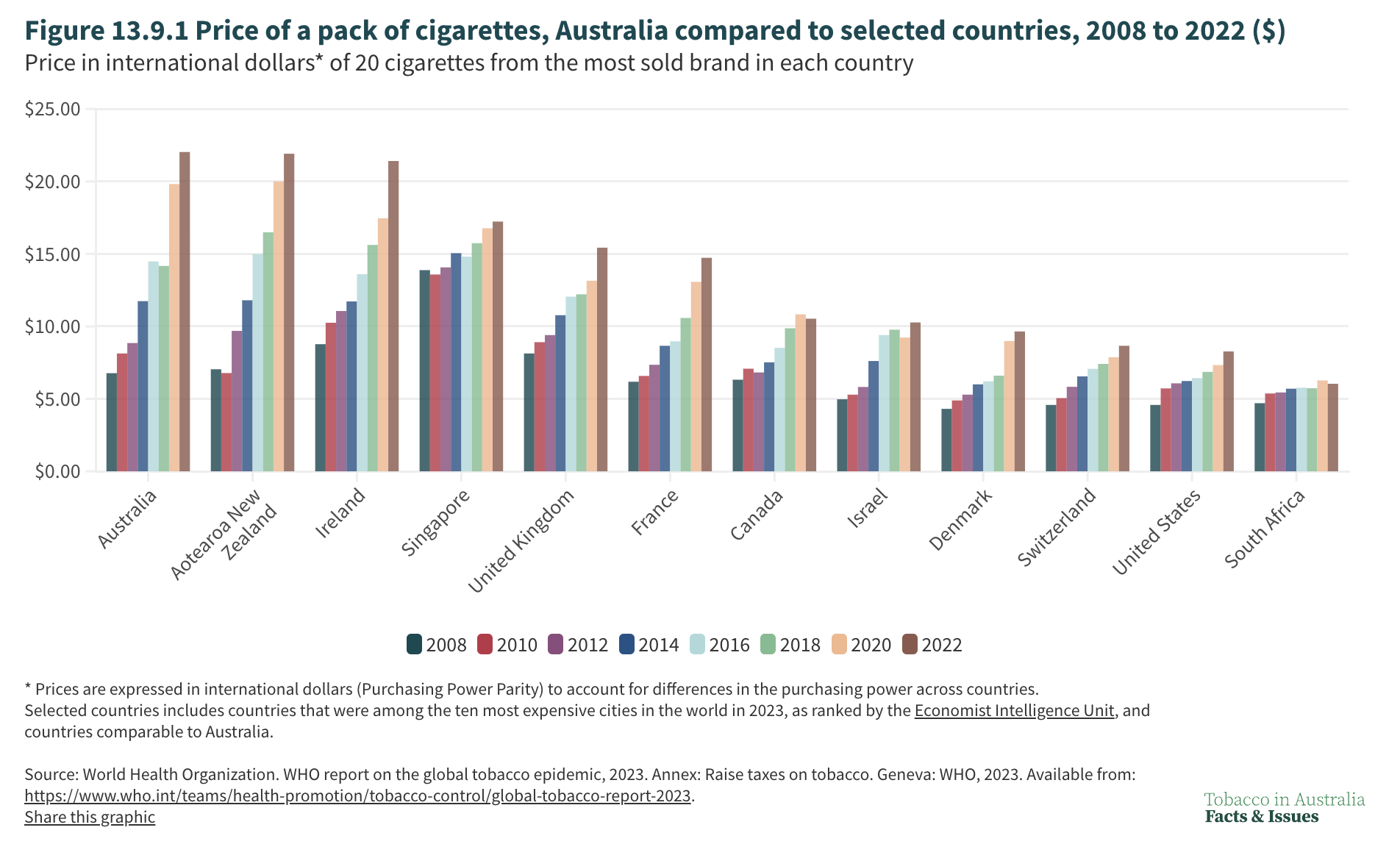
Vaping may well be a factor helping adult smoking cessation in both countries, although both nations also have the world’s highest retail prices, advanced comprehensive tobacco control policy and enjoy widespread public support for further government action. Recent data shows 94.6% of New Zealand smokers were aware of the Smokefree New Zealand proposal, with 77.8% of smokers and recent ex-smokers supporting the Smokefree Generation proposal and 73% supporting the denicotinisation of cigarettes.
When the price of cigarettes between the two countries is standardised to international dollars, cigarettes in New Zealand are the least affordable in the world in 2022. Might not this have had a little something to do with so many smokers quitting in New Zealand?

Collateral damage to youth
There has also been significant collateral damage in the form of re-ignition of nicotine addiction among former-smokers and starting it in many who had never smoked. A recent large (n=31,733) US cohort study assessed smoking and vaping transitions between two waves (2016-2017 and 2018-2019) and found for every beneficial transition out of smoking via vapes, there were 2.1 harmful transitions (ie never smokers starting to vape, exclusive vapers taking up or adding smoking to vaping). So the net population effect of vaping may well be negative.
Here, teenage vaping data is of particular interest. A New Zealand Ministry of Health analysis of pooled data from 2020/21 and 2021/22 for 15-17 year olds found 76% of daily vapers had never smoked, 18% were former smokers and 6% were dual users [24]. The latest wave of data from Australia’s GenVape study show that 50% of current vapers (last 30 days) had never smoked. (unpublished data provided by GenVape)
When smoking prevalence is very low in youth (as in the five nations discussed above), the argument that high vaping prevalence might be substituting for more widespread smoking is difficult to sustain against a background of plummeting smoking prior to significant uptake of vaping. Daily vaping rates in 14-15yr Australian, New Zealand and US students are 2.8%, 10% and 3.5% respectively, and in 15 year olds in Canada 8.1% and 10.9% in English adolescents. Daily smoking rates have been below those figures for some time.
Concern about youth vaping has mostly been about vaping priming some for subsequent smoking, as well as about the financial and health burdens of nicotine dependence in itself (eg: on-going expense, social inconvenience, possible neurological and major psychiatric problems and possible cancer promoting action). As 15 presidents of the Society for Research on Nicotine and Tobacco wrote in 2021 “There are no data on long-term health effects, reflecting the relative novelty of vaping and the rapid evolution of vaping products. Determining even short-term health effects in adults is difficult because most adult vapers are former or current smokers.”
Benefits of prescription drug access
Australia’s pharmacy-only access model harnesses the benefits of providing easy access to vapes by adult users and minimising collateral damage to children. Argument that accessing vapes through pharmacies is onerous is particularly silly. Some 5935 community pharmacies are located throughout the country, with at least one in every shopping mall, and in all but the smallest shopping strips in suburbs and in towns throughout regional Australia. In capital cities, 97% of people live within 2.5 kilometres of a pharmacy, and 66% live within 2.5 kilometres in the rest of the country. Over 2000 are open after hours and at weekends. Telepharmacy and postal delivery service those in remote areas. The Pharmacy Guild estimates that in 2022-23 there were 443.6 million individual pharmacy visits. In a population of 27 million, 335.8m prescriptions were dispensed for all drugs. Many more across-the-counter purchases would have additionally occurred, as can occur with 20mg or less vapes now without any prescription.
The prescription model of access to drugs with misuse or abuse potential has flourished for decades in all but lawless or chaotic nations where almost any drug can be obtained without a prescription. Criminal gangs have not decided that Australia presents a golden opportunity to supply any of the 925 Pharmaceutical Benefits Scheme drugs to millions of people wanting them cheaper and without the inconvenience of getting a prescription.
In Australia, there are black markets for some pharmaceuticals including anabolic steroids, some new and expensive weight-loss drugs and erectile dysfunction drugs, but these are very marginal compared to the overwhelming supply volume via prescription access through pharmacies. A BBC report detailed criminal gangs diverting a range of prescribed drugs in England. Black markets do exist for prescribed drugs but the size of these are a tiny fraction of those which operate via prescription access.
