
At different times during the COVID-19 pandemic, Australian states and territories have mandated mask wearing in various public settings. As I write this on Feb 1 2021, my own state of NSW currently mandates masks in the Greater Sydney region (including the Blue Mountains and Northern Beaches), the Central Coast and Wollongong). Masks must be worn on public transport, for staff in hospitality settings (bars, restaurants, cafes), in hairdressing salons and barbers, beauty parlours and nail bars, massage parlours, tanning salons, on planes and in airports, and at places of indoor worship, weddings and funerals.
Those breaching these rules can be fined $200 (individuals), $1000 for small business owners not enforcing mask use and $5000 for corporations.
During most of January, this list also included all shops. The future may see changes to these rules, depending on infection rates and locations.
Health workers and many citizens were vociferous advocates for masks to be made mandatory from the early days of the pandemic. But without their use being mandatory, voluntary rates of adoption were depressingly low. In late July 2020, out of curiosity I took myself off to my local railway station for 90 minutes in the morning commute period with two hand counters, clicking with one hand all those boarding or alighting wearing masks, and with the other, those not wearing masks. Nearly 93% were maskless.

When Sydney’s northern beaches experienced a significant cluster which threatened to spread beyond the locked down peninsula, the state government relented and rapidly mandated masks in all indoor settings and on public transport from midnight on January 2, 2021.
It was obvious to all that there was an immediate, almost 100% compliance that lasted until the relaxation announced several weeks later.
As I blogged earlier, this was almost entirely predictable, mirroring the 100% compliance with a restaurant indoor smoking ban when it was first introduced in time for the Sydney Olympics in 2000, compared with the situation in Melbourne which at time still allowed smoking in restaurants.
There is a huge, unassailable lesson in this. Public information and persuasion campaigns designed to motivate people, manufacturers and the service sector to voluntarily adopt behaviours or changes in the way they manufacture or provide good and services will get you only so far.
When you face deadly serious threats to large numbers of people, and voluntary appeals are not translating into widespread adoption, legislation backed with fines can make a huge, sometimes instant difference. Harvard University’s David Hemenway documented many examples of this in the injury and violence prevention in his 2009 book While we were sleeping: success stories in injury and violence prevention.
And the view from behavioural science research?
I was motivated to write this blog after reading a paper by a group of English behavioural scientists “Interventions to increase personal protective behaviours to limit the spread of respiratory viruses: A rapid evidence review and meta-analysis”. They have put it out for open review: anyone can publish their comments on the open-access website.
I could scarcely believe what I was reading as I made my way through their painstaking analysis and synthesis conducted between July-December 2020. They gathered studies examining how “interventions” affected changes in hand hygiene, avoiding touching the ‘T-Zone’, catching droplets in tissues face mask use disinfecting surfaces and maintaining physical distancing.
Here, I’ll just focus on their mask wearing results. They located just 12 studies examining what happened when people are exposed to interventions intended to increase mask use. Their conclusions? “mixed results, with three studies reporting positive effects, two studies reporting no difference, one study reporting negative effects and six studies with indeterminate results.”
And their concluding implications? The few and often low quality of the studies suggest “a missed opportunity for harnessing techniques indicated by relevant behaviour change theory and evidence. We encourage policymakers and healthcare practitioners to work collaboratively with behavioural scientists to incorporate techniques that theory or evidence predicts are effective for enabling personal protective behaviours, such as techniques targeting motivational or self-regulatory processes.”
So all clear, are we, about what behavioural change research offers policy makers hungry for information about how to increase mask use?
It appears that the authors made a rod for their own back by limiting what “interventions” they should include in their review. Call me picky, but to my mind a law requiring everyone to wear a mask at risk of a fine, combined with the massive news reportage that invariably accompanies the introduction of such laws, ubiquitous posters reminding people about masks and frequent railway station platform announcements, might just count as an intervention a tad more important than some little study of what happens when some university students were sent free masks to prevent acquiring influenza.
In an August 2020 publication by the Council on Foreign Relations, “more than half” the world’s nations had mandated either total public space mask use or use in certain areas or circumstances. A graph in the report (below) showed very wide differences across nations in those self-reporting that they had worn a mask outside the home on the last seven days. Self-reported data on an issue like masks that attracts sometimes significant opposition is unlikely to have high reliability, compared with direct observation of mask wearing rates.
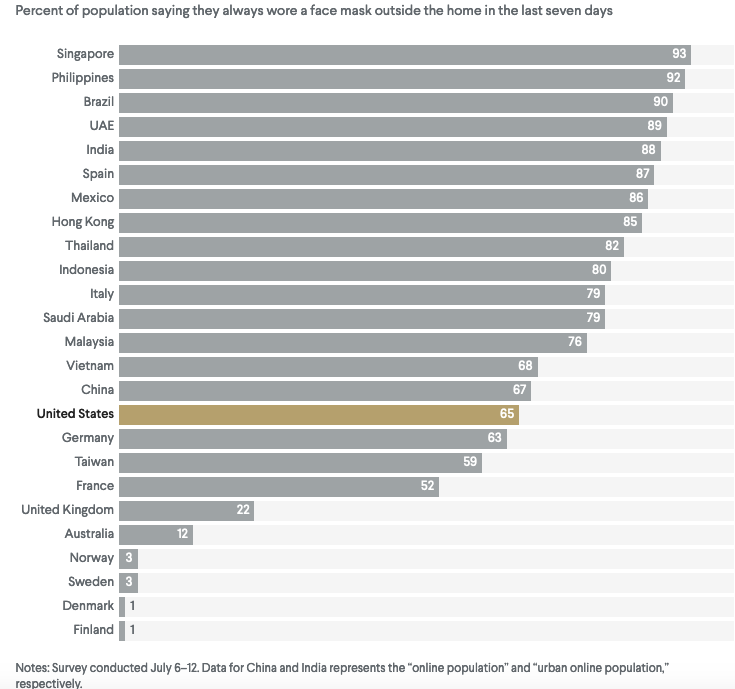
It is likely that there are widespread cultural differences that are highly relevant to mask use, which go beyond simple questions of whether masks are mandatory or not. Many Asian cultures have a long standing tradition for those with respiratory symptoms to wear masks. Differences in enforcement rates will also be important, as will those in a nation’s overall tendency in its citizenry to obey public laws.
This law in NSW produced a blindingly obvious, nearly universal uptake in mask wearing in all areas which required it. So the absence in this review of even a mention of such massive impacts on mask use was startling.
I searched PubMed for studies on the prevalence of mask wearing during COVID. I found many papers reporting and reviewing experimental evidence on the reduction of aerosol from mask wearers, and some papers comparing COVID 19 incidence rates in states and districts which mandated masks compared with those which didn’t (see here for example). But I found no papers showing time-series data comparing the prevalence of mask wearing before and after the introduction of mask laws.
Observational data like this are commonly collected and published in the monitoring and evaluation of the impact of a wide variety of public health laws and regulations like restaurant smoking, car roadworthiness, seat belt and infant restraint use in cars, blood alcohol and cannabis levels in drivers, helmet wearing by motorcyclists and cyclists, cockroach and rodent infestation in restaurant kitchens, and indoor air quality in workplaces. These are just a few examples.
If I’m right that there are few or no studies of mask uptake after the passage of laws mandating this, the researchers whose paper I described above could be forgiven for not including any in their review. COVID-19 is the largest health threat that all alive today have ever faced. All governments urge their citizens to wear masks, yet many still do not mandate it. Data clearly in plain sight for all of us to see that mandatory masks massively increase mask use could very easily be “upgraded” in evidence status by properly conducted surveillance studies. Such data would be invaluable in levering tardy governments into mandating their use.
