

Following the publication of my new open access book Quit Smoking Weapons of Mass Distraction (Sydney University Press) I’ve been speaking to thousands of Australian GPs at conferences around Australia about vaping. The book includes a 16,000 word chapter looking at hype about vaping. My talk to the GPs focuses on 10 cornerstones of what I call “vaping theology” – beliefs that all vaping true believers hold to be inviolable. The Medical Republic published a lengthy piece summarising my Sydney talk.
Dr Colin Mendelsohn, or the folksy “Dr Col” as he likes to call himself these days, is Australia’s Energizer Bunny of vaping promotion. He didn’t like what he read and took to his blog to provide us with a “detailed …more scientific analysis”, giving himself a giant tick.

Let me take apart his sophistry one claim at a time. A warning, this won’t be pretty.

Response: I’m very sorry Dr Col, but it is true. The 2014 paper reported on a consensus of 12 people convened by the hyperbolic Prof David Nutt in 2013. They rated 12 nicotine containing products for harm and judged vaping as having 5% the harm of cigarettes, after acknowledging “A limitation of this study is the lack of hard evidence for the harms of most products on most of the criteria”. Just read that again. Caveats don’t come more sweeping than that. So this was a estimate not worth a cracker.

But I am wrong about the provenance of the figure says Dr Col: he says the 95% figure came from the 2016 report of the Royal College of Physicians (RCP) and the now defunded Public Health England’s (PHE) 2014 report and 2015 update, both written after the Nutt paper.
In this 2019 blog, I forensically searched the RCP and PHE reports for the evidence informing the 95% figure. Nowhere in either report is there any worked calculation of the 95% factoid, which with others I shredded in the American Journal of Public Health in 2020. But in both reports, all referencing roads lead back to the Nutt report.
Dr Col’s blithe “not the point” dismissal of the lack of precision about the relative toxicity of vaping and smoking would amuse any toxicologist. Strychnine is less dangerous than cyanide. Proximity to sharks less dangerous than sharing a room with someone with Ebola. The point though, is that all deserve the utmost caution, not that we frame the choice as one or the other. How about quitting smoking and vaping?

Response: Dr Col always calls for vapes to be openly sold as “consumer products”, just like ordinary grocery items including cigarettes. With the support of nearly every health authority and NGO in the country, the Australian government has instead commendably restricted legal access to nicotine vapes to those with prescribed authority to access them through a pharmacy.
All new pharmaceutical products are scheduled by the TGA to enable tracking of prescribed use and reporting of adverse events. These reports over the years see drugs rescheduled up or down (sometimes including bans) in response to data on any problems found with short or long term use. Many vaping advocates argue strenuously against vapes being prescribed, invoking the urgent duty to save millions of lives. But advocates for life-saving drugs for cancer, HIV-AIDS and heart disease don’t think their drugs should be available over the counter in corner shops. Vaping advocates seem to think their issue is far more important than any other therapeutic good.

Response: There is in fact a large research literature about the roles of nicotine in a wide range of disease processes. I captured some important examples of this here, including disturbing emerging evidence on nicotine as a possible cause of schizophrenia and as a promoter for several cancers.
The role of the vasoconstrictor nicotine in cardiovascular disease has long been known, and with unregulated flavoured disposable vapes flooding many world markets and providing as much nicotine in some vapes as in 9 packets of cigarettes, nicotine is by no means some benign vitamin-like substance that vaping theology insists.
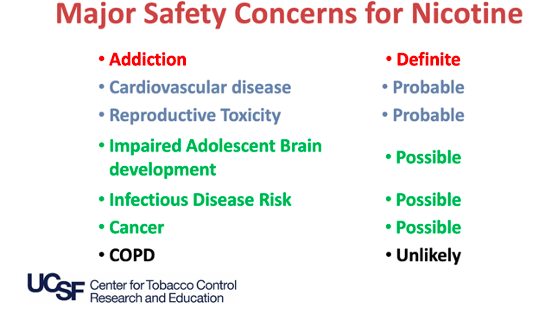
Neal Benowitz, arguably the world’s foremost nicotine pharmacologist, summarised current awareness of nicotine safety risks in a presentation to the annual nicotine/vaping conference in Warsaw in 2019 (see his slide below). In only one area (COPD) was there any assessment matching Dr Col’s assertions.
Dr Col has previously pilloried evidence about vaping toxicity from animal studies. But as a prescriber he’d be well aware that the standard LD50 metric (Lethal Dose required to kill 50% of exposed laboratory animals) is used globally to rate the toxicity of chemicals. He’d also be aware of the vast record of animal studies being used in the development of safety and efficacy of many life saving drugs.
Yet when it comes to inconvenient information about possible negative effects on adolescent brain development, vaping theologians instinctively wave the dismissive “pure speculation” flag.
This recent longitudinal study of very young children who used any form of nicotine found, using neuroimaging outcomes, “a significant association was found of early-age initiation of tobacco use with lower crystalized cognition composite score and impaired brain development in total cortical area and volume. Region of interest analysis also revealed smaller cortical area and volume across frontal, parietal, and temporal lobes.”
Nothing to see there, Dr Col?
Response: Dr Col writes that flavours encourage uptake of vaping “by current smokers” in the same way that they do with NRT gum and lozenges. Errmm … there are two rather large issues carefully omitted here. Vaping involves inhaling vapourised chemical flavours, while NRT flavours via gum and lozenge are ingested. In this blog and my book, I set out in detail why it is that no inhaled pharmaceuticals are flavoured (such as asthma puffers) and why the US flavour and extracts manufacturing industry (which stands to make billions if governments gave the green light to flavours in vapes) has spoken strongly against flavours in vapes.
And then there’s the teensy little issue of the huge attraction of flavours to nicotine naïve children who are flocking to vaping all over the world, and the importance of flavours in predicting on-going vaping. Why did you omit this, Col?

Response: Sadly, Dr Col apparently did not attend my talk, so has completely misunderstood what I actually spoke about here. I showed data from the UK government’s annual Opinions and Lifestyle Survey showing that the average number of cigarettes smoked daily by smokers who vape (8 a day) is almost identical to that by smokers who have never vaped (8.1 a day).
But in any case, his selective summary of dual use is a cherry-picked special. Dual users are also exposed to more toxins than cigarette smokers and dual use does not predict smoking cessation, as shown in this 4 nation study where “smokers with established concurrent use [smoking and vaping] were not more likely to discontinue smoking compared to those not vaping … it is clear that the rates of transitioning away from smoking remain unacceptably low.”

Response: Again, Dr Col responds to something he’s guessing I was talking about here. What I actually spoke about was the bankruptcy of the so-called hardening hypothesis. Dr Col’s response indicates he’s fully signed-on to the idea that today’s smokers are predominantly those who “can’t” quit. The US smoking cessation maven John Hughes reviewed 26 studies which examined the hardening hypothesis to see if this was true. Hs conclusion? “Some have argued that a greater emphasis on harm reduction and more intensive or dependence-based treatments are needed because remaining smokers are those who are less likely to stop with current methods. This review finds no or little evidence for this assumption.”
Response: My book has a section of a whole, large chapter (#2) explaining why participants in smoking cessation RCTs bear scant resemblance to those from real world longitudinal use. Just to take one example, two thirds of smokers would not be deemed eligible to enrol in an RCT. Reasons here include mental illness, which is much higher in smokers. Such ineligibility will mean that RCTs are likely to be strongly biased to not include many deeply nicotine dependent smokers. My chapter also explores many other issues that differentiate the attention paid to RCT participants by researchers compared with how cessation products are used in the real world.
And yes, meta-analyses of RCTs like Cochrane do find that vaping is more successful than NRT. But the “success” here is utterly, stonkingly dismal. Ninety out of 100 smokers assigned to vaping in RCTs continue to smoke, compared with 94% using NRT. Is there any other drug in the whole of medicine that would attract the epithet “successful” with a failure rate of 90%?
Longitudinal cohort studies of smokers who vape also reach conclusions that vaping is far more dismal than disruptive, with plausible concerns that it may hold more in smoking than it tips out of it. Again, my book discusses this at length.
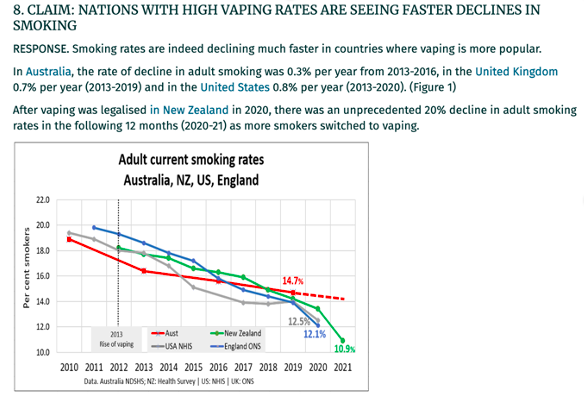
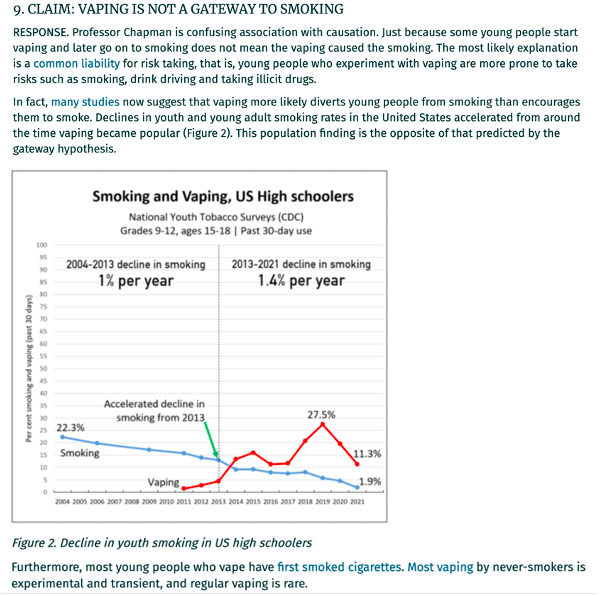
Response: Oh dear, Dr Col is at it again. He’s using data in August 2022 that is way out of date. In this blog I wrote in April 2022, I explained how the dotted line you see in Col’s graph above for Australia is now down to 11.8% (if we take all smoking …even very irregular smoking … into account) and down to 10.7% for daily smokers. That’s because we have 2021 Australian data, which unfortunately don’t fit Col’s narrative so he leaves it out. Australia is just behind New Zealand (on just one year’s data), but ahead of the UK and USA.
Response: Debate about whether vaping leads (ie increases the likelihood) to smoking or whether it’s simply a matter of “kids who try stuff, will always try stuff” (dignified as “common liability theory”) will always be on-going because it will of course never happen that children will be randomised to vape or not vape and then followed up for several years. The best we can do is to look at large cross-sectional cohorts and control in analyses for the very factors that common liability theorists say confound claims that vaping leads to smoking.
The best example of this is a paper on the UK’s huge Millennium Cohort. It found “Among youth who had not smoked tobacco by age 14 (n = 9,046), logistic regressions estimated that teenagers who used e-cigarettes by age 14 compared with non-e-cigarette users, had more than five times higher odds of initiating tobacco smoking by age 17 and nearly triple the odds of being a frequent tobacco smoker at age 17, net of risk factors and demographics.”
Very importantly, the paper also knocked the stuffing out of the glib ‘kids who try stuff, will try stuff’ common liability dismissal of the concern that vaping acts as training wheels for later smoking uptake. In their analysis the authors controlled for a rich constellation of ‘propensity’ factors that have been suggested to predict smoking uptake in youth. These included parental educational attainment and employment status; parental reports of each child’s behaviour during the prior 6 months using the Strengths and Difficulties Questionnaire, with indicators of externalizing behaviours (i.e. conduct problems, hyperactivity, inattention; and internalizing behaviours (i.e. emotional symptoms, peer problems) parental smoking; whether a child spent time ‘most days’ after school and at weekends hanging out with friends without adults or older children present. Children, via confidential self-reports, indicated whether they had ever drunk alcohol (more than a few sips), ever engaged in delinquency (e.g. theft, vandalism) and whether their friends smoked cigarettes.
The authors concluded:
“we found little support that measured confounders drove the relationships between e-cigarettes and tobacco use, as the age 14 e-cigarette and tobacco cigarette estimates barely changed with the inclusion of confounders or in matched samples. Furthermore, early e-cigarette users did not share the same risk factors as early tobacco smokers, as only half the risk factors distinguished e-cigarettes users from non-users, whereas age 14 tobacco smokers were overrepresented on almost all the antecedent risk factors. If there was a common liability, we would expect similar over-representation for users of both forms of nicotine.”
And as for Col’s statement “Most young people who vape have first smoked cigarettes”, I’ll just leave you with this. In the 2019 New Zealand Youth Survey, “More than 80% of ever-vapers (N=2732) reported they were non-smokers when they first vaped, and 49% of regular vapers (N=718) had never smoked.”

Response: Do you all see what Dr Col has done here? He’s highlighted data in Philip Morris International’s second quarterly report for 2022 about the growth in revenue it’s getting from its putative reduced risk products. Premium products have long been far more profitable per unit for tobacco companies than budget products like much cheaper cigarettes. But in public health, we are more interested in how much of which products the tobacco industry is selling, not how much money they might make from each. Col might have missed this graph in the same report.

And from earlier in the year

With this brilliant observation

So, PMI’s much trumpeted drive to reduce consumption of its ultra-deadly cigarettes is, in their word, “recovering”. In Philp Morris-speak, the decline in cigarette use is now reversing at the same time as its pricey heat sticks are increasing. So much then for unsmoking the world, particularly in Poland, Turkey and Indonesia where cigarette shipments are increasing.
